
April Meeting, 1942
A STATED Meeting of the Society was held, at the invitation of Mr. Zechariah Chafee, Jr., at the Tavern Club, No. 4 Boylston Place, Boston, on Thursday, April 23, 1942, at half after eight o’clock in the evening, the President, Kenneth Ballard Murdock, in the chair. By invitation of the Council, members of the Massachusetts Historical Society attended the meeting.
The records of the last Stated Meeting were read and approved.
The President reported the receipt of letters from Mr. Charles Cortez Abbott and Mr. Robert Peabody Bellows accepting election to Resident Membership in the Society.
Mr. Richard LeBaron Bowen and Mr. George Norton Northrop were elected Resident Members, and Mr. Daniel Joseph Boorstin and Mr. George LaPiana were elected Associate Members of the Society.
The President appointed the following committees in anticipation of the Annual Meeting:
To nominate candidates for the several offices,—Dr. Harold Bowditch and Messrs. Robert E. Peabody and Elliott Perkins.
To examine the Treasurer’s accounts,—Messrs. Allston Burr and Hermann Frederick Clarke.
To arrange for the Annual Dinner,—Messrs. Augustus Peabody Loring, Jr., and William Vail Kellen and Dr. James L. Huntington.
Some Common Diseases of Colonial Children
THIS paper concerns only seven of the two thousand diseases that were known to the physicians of Cotton Mather’s time. These seven have been studied as a group because they were all common contagious diseases and therefore responsible for many, if not most, of the colonial epidemics. So far as children were concerned, two of these diseases, chicken pox and mumps, were relatively harmless; but another two, diphtheria and dysentery, outranked smallpox as a cause of death. I have not included smallpox because its history in America is already fairly well known.
These notes were assembled with different classes of readers in mind. For general historians who, no doubt, have long been familiar with colonial epidemics, I have endeavored to eliminate unnecessary medical terminology in order to make this important, though morbid, aspect of colonial social life less bewildering than it appears in the original medical publications. For epidemiologists who may be interested in whether or not contagious diseases change in character over a period of years I have attempted to appraise the severity of some epidemics by citing the most important available statistics. I have also had in mind those young physicians who, on first becoming interested in medical history, are usually unaware of the vast amount of American material yet to be explored. They should not be discouraged because American medical books contributed so little to the advancement of medical science; but if truly interested in the history of their profession, they will find that colonial newspapers, sermons, letters, proclamations, and the like, although written by and for laymen, often contain important medical facts. Even casual observations on diseases in the diaries of observant laymen are frequently more instructive than the best of nebulous theories. Every historical library has at least a few church records, bills of mortality, physicians’ letters, or original descriptions of diseases awaiting modern medical interpretation. Colonial America produced no Harvey, Sydenham, or Jenner, but it had its share of diseases; and a medical history of a country should include not only the biographies of its doctors but also the histories of the diseases which they tried to conquer.
Measles1
1657–1658
According to John Hull, measles broke out in Boston and surrounding towns during September and October, 1657. By November it had spread to Hartford; and during the winter it continued to spread throughout the Connecticut River valley and also along the southern New England shore at least from Stonington to Stamford. Thomas Minor’s diary, the Winthrop family correspondence, and especially the younger John Winthrop’s medical records reveal that adults as well as children were afflicted, so it is reasonable to suppose that this was the first measles epidemic in New England. Many of the patients suffered complications yet, on the whole, the epidemic was not very severe for out of a large number of cases in Boston “scarce any died of it.”2
1687–1688
Thirty years later, measles broke out again in Boston, and during the winter of 1687–1688 it “raged throughout the country.” At about the same time “the King’s ships brought the Measles” to Quebec. In contrast to the first one, these epidemics appear to have been severe. No statistics are available, but of five adult cases mentioned in one brief passage in Sewall’s diary, two were fatal. It also appears that inflammation of the brain (encephalitis), the most serious of measles complications, was fairly common, particularly among adults. There are some indications of it in two of Sewall’s letters; and Joshua Moody wrote to Increase Mather: “There are also sundry in the Country that remain distracted since the measills last spring.”
1713–1715
Several persons died during an epidemic in Virginia during 1693, but there is no available evidence that this epidemic spread to other colonies. During the late summer of 1713 the disease appeared in some town near Newport, Rhode Island, and from there it was apparently carried to Cambridge by some Harvard student, for an epidemic broke out at the college during September before it spread throughout the town. The Boston epidemic began during October and continued until the following spring. By January the disease had reached New York and a few towns in New Jersey, and by March it had appeared in numerous towns from Piscataqua to Philadelphia.3 The epidemic passed by some towns at first only to return to them some months later. It was present on Long Island during May, 1714, on Cape Cod during June, in Danvers during November, and in New London during the winter and spring of 1714–1715.
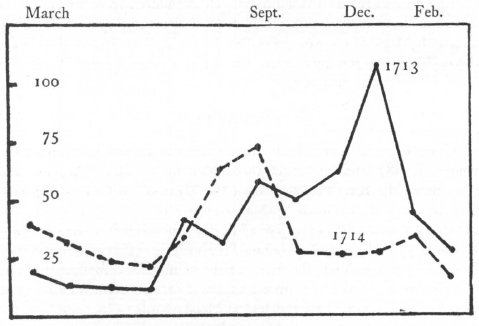
Deaths in Boston, 1713–1714
During an average year (1714) the peak was reached in September.
This was the most alarming measles epidemic of colonial times. It was particularly severe in Boston, for “The Hand of the Lord was heavy there.” Out of a population of about 9,000, “Many Hundreds, perhaps Thousands,” had the disease.4 Compared with the same months of the following year, there were 180 excess deaths;5 so it is safe to attribute at least 100 to the epidemic. Three different fast days were observed during the winter of 1713–1714 because of measles, scarcity of corn, and “General Adversity”; and about the first of April there was “Publick Thanksgiving . . . for God’s Great Goodness . . . in restoring Health.”6 This epidemic was also severe in other towns. During March it was “very mortal” in Salem, West-Jersey; and on May 27 it was reported from Philadelphia: “We have here an extream sickly Town, and many Dies, five lies Dead now, and several were Buried Yesterday.”7 In New London there were nine measles deaths in a population of 2,000. A minister in Westchester, fearing that he would get the “very mortal distemper,” refused to baptize a dying child.
Cotton Mather repeatedly said that in Europe measles was usually considered a mild disease, but that in America it was “a very heavy Calamity; a Malady Grievous to most, Mortal to many, and leaving pernicious Relicks behind it in all.” He had good reason “to Remember the Wormwood and the Gall,” for every member of his household except himself got this “venomous” disease, and five of them—his wife, maid, newly born twins, and two-year-old daughter—died within two weeks. Another daughter, Katherine, never regained her health after her attack, dying three years later at the age of twenty-seven from a residual “consumption.”8 Three children in one family and two in another died during the New London epidemic. It should be stressed that this was one of the very few measles epidemics during which there were multiple deaths.
As in other epidemics, there were some exceptions to the general rule. Of the first fifty scholars who were sick at Harvard College, every one recovered.9 The diaries of Joseph Green, Joshua Hempstead, and John Pain reveal that though the disease was undoubtedly more severe than usual, many families pulled through without serious complications. Also, in spite of measles being exceedingly contagious, some families in Boston managed to escape it entirely.10 In small, distant towns many more families must have escaped also, because, as the records of subsequent epidemics show, many persons living in 1713 did not get the disease until they were advanced in years.
Inasmuch as measles is still frequently confused with other diseases, one must consider the possibility of error in those cases called “measles” in nonepidemic years of colonial times; but, on the other hand, the disease having been so alarming and so many persons having made determined efforts to avoid it, it is possible that many successfully escaped epidemics only to get the disease when off-guard in nonepidemic years. At any rate, after the epidemic of 1713–1715 more cases of “measles” can be found than after any other serious and widespread epidemic. A death from measles was said to have occurred in New London in January, 1716,11 a year after the epidemic swept through that town; and John Legg of Boston said that his family had it about February, 17 16, which was then “a time of general health.” There was at least one case of “measles” in Dedham in 1717;12 and another epidemic was reported in Hingham in 1722.13 There had been an epidemic on board a ship from Ireland which arrived in Boston harbor in 1724. The failure of widespread epidemics to develop from these cases is best explained on the ground that not enough susceptible persons were congregated in any exposed area for an epidemic to get started. It is also interesting that following this epidemic, everyone fully appreciated the value of permanent immunity. Periodically in the newspapers appeared advertisements of the sale of slaves whose owners thought they were all the more desirable because they had had “the Measles and the Small Pox.”14
No account of the 1713 epidemic would be complete without a word about Cotton Mather’s A Letter about a Good Management under the Distemper of the Measles, at This Time Spreading in the Country. Although at one time dismissed as merely “an ancient curiosity,” it happens to be, particularly because of its originality, one of the very few classics of early American medicine.
1729
The epidemic of 1729 appears to have been more severe in some towns than in others. So far I have found records of only three measles deaths in New England—one person died in New London in February at the age of sixty-four, another in Guilford in June at the age of thirty-six, and another in Lynn in July at the age of twenty-six.15 The May epidemic in Boston was “very favourable & moderate.” The New York epidemic was very serious probably because it occurred at a time when pneumonia (or influenza?) was prevalent. During March and April there were “numbers of buryings, Some of the measles but most of the pain in the side.” By proclamation the Governor suspended the sessions of the Supreme Court for over two months to help prevent the spread of the “infection in the air.”16 “In all my days,” wrote James Alexander when many members of his family were having the disease, “I never saw So generall a Sickness in a place nor a greater Mortality.”
1739–1740
Though Thomas Smith mentioned an epidemic in Falmouth during the summer and autumn of 1736, the next large epidemic in New England broke out in 1739. It started in Boston in June and apparently continued at least until November when Cotton Mather’s Letter was reprinted. During November it broke out also in Lynn17 as well as in Natick where two children of Hezekiah Comacho, an Indian, died.18 The Reverend Ebenezer Parkman mentioned that the disease was in Shrewsbury during July, in Springfield during November, in Westborough and Southborough during December, and in Marlborough and Worcester the following March.19 Parkman’s account is doubly interesting because of his mention of many adult cases, including those of his own wife and “old Mr. Fay” and his wife, and his description of Silas Brigham, thirty years old, who was “raving Distracted” (from encephalitis?) for at least three weeks after his attack. There were many multiple deaths, but they were apparently all caused by throat distemper, which was raging throughout Worcester County at that time.
In Connecticut there were epidemics in New Haven, New London and Hartford. Some students at Yale had it in January, 1740. The three victims in New London were 14, “60 odd,” and “about 72 or 73” years of age.
1747–1749
On the basis of some figures in the Births and Burials for Christ Church Parish, Philadelphia, it is estimated that there were 84 deaths from measles among the 15,000 inhabitants of that city during 1747. That makes a measles death rate of 560 per 100,000 population, which seems extraordinarily high compared with the present rate of about 0.3 per 100,000.
Only a few scattered notes are available concerning the disease in New Hampshire,20 Massachusetts,21 Connecticut, New York, Pennsylvania and South Carolina.
1758–1760
The epidemic which began in 1758 continued into January, 1760. Records of it have been found in about twenty-five towns from Maine to South Carolina.22 It was “very thick” in Cambridge, and because so few at “the seat of the Muses” had had the disease, the winter vacation was prolonged three weeks. Nevertheless, “pritty many Scholars” came down. The vital records of various towns show a fairly large number of infants, wives, and widows dying from the disease. Some very prominent persons had it. Henry Gibbs, Clerk of the Massachusetts General Court, died in February, 1759. Mrs. George Washington, then twenty-eight years old, caused her husband a little uneasiness for a few days but apparently recovered without complications.23 William Tompson, minister at Scarborough, died at the age of sixty-two and was buried by the town with pomp and splendor at a cost of £22.24
This epidemic, in particular, illustrates the risk of drawing false conclusions about the severity of measles from records of local epidemics. “Several” died in Falmouth out of a population of less than a thousand. At least five of the nine hundred inhabitants of Medford died. The Reverend John Ballantine of Westfield wrote in his diary for April 18, 1759: “The measles have been in every house but six or seven in town. Many have died, nine in April, one child lost the sight of one eye.”25 In Fairfield, New Jersey, not a family was spared, and “many” died. It is estimated that there were over one hundred deaths in Philadelphia. One might therefore conclude that measles was unusually severe in 1759, but in Marlborough, Massachusetts, out of a population of about twelve hundred there were over five hundred cases “from the Age of Seventy-odd to the Age of six Weeks, and not one Person died.” Also, in his Thanksgiving Proclamation, the Governor of Massachusetts said that, on the whole, the visitation had been “so gentle.”
1772–1774
The next great epidemic is interesting in view of the relation of measles epidemics to wars. In the army camps of the first World War, the Civil War, and the War of 1812, measles caused considerable trouble; but the medical records of the Revolutionary War have, so far, failed to reveal any trace of the disease. This was because the epidemic which started in 1772 and which was still spreading on some isolated plantations of Virginia in February, 1774, had involved all the colonies, at least from Maine to South Carolina,26 and had left the population immune. Like many other epidemics, this one varied in severity in different towns and also involved all age groups, though these features were not so striking as in previous cases. By August, 1772, when the disease had reached its peak in Boston,27 it had been “very light,” and in November the Governor proclaimed a Day of Thanksgiving, among other reasons, because “an infectious Distemper which had sometimes been very mortal and grievously distressing was then mild and gentle.”28 By the following January, in the North Parish of Bridgewater, out of an estimated population of less than a thousand, there were 721 cases and four deaths.29 There were nine deaths among the 8,000 people of Salem,30 and about 150 deaths among the 25,000 people of Philadelphia. In Ipswich one infant died aged seven weeks and another aged three months;31 while at the other extreme, a widow “above 70” died in Gloucester, and Mr. Nathan Packard, “upwards of 80 years of age” died in Bridgewater. Stephen Scales of Chelmsford died from an “apoplectic seizure after measles” (encephalitis?) when thirty-one years old.32 It was said that the disease spread from the northern colonies to Charleston, South Carolina, where eight to nine hundred children died,33 but these figures are so far out of line that they need to be confirmed before they can be accepted. There was also a report of a terrible epidemic of “flux” which caused six to seven deaths daily in Williamsburg, but the Virginia Gazette of July 22, 1773, reported “with the utmost pleasure . . . that what gave rise to it is only a disorder incident to children after having had the measles.”
1783, 1790, etc.
Though more details are known, there is very little to add about epidemics after the Revolution except that in the larger cities, such as Boston, New York, and Philadelphia, they occurred at intervals of five to seven years. In Philadelphia there were sporadic deaths from measles almost every year after 1795; but whether the disease had become endemic or whether some of those deaths were erroneously attributed to measles cannot, of course, be determined now. The same may be said for Boston after 1821. At all events, by the turn of the nineteenth century measles had become primarily a disease of childhood, though one can find deaths here and there in persons over thirty years of age.
A review of measles epidemics in any one town reveals a steady, almost mathematical, reduction in the interval between them. I select Boston to illustrate this interesting sequence because it so happens that my Boston records are the most complete. From 1657 to 1841 the interval in years between epidemics was as follows:—30–26–16–10–8–12–13–11–7–7–5–7–6–6–4–4–3–3–6. This gradual reduction in time over the course of two centuries was the result of three interrelated factors: the sailing time between Europe and America, a steady increase in the number of ships and passengers, and a gradual increase in population density.
Up to 1657 the Atlantic Ocean was an effective barrier against measles in spite of epidemics in England, or at least in London, at intervals of three to five years.34 Since during the seventeenth century the average sailing time was eight to ten weeks and the incubation period of measles less than two weeks, it follows that most shipboard epidemics must have burned out before the ships could reach these shores. To explain the two seventeenth-century epidemics it seems necessary to assume measles epidemics aboard fast ships each with at least one susceptible person so isolated that he could escape the disease until a few days before debarkation. That such coincidences must have been rare explains why epidemics were infrequent. It is possible, of course, that the disease could have been imported from the West Indies; but without any material concerning epidemics there, I surmise that they were few and far between because, for the same reason, the ocean should have protected that area too. During the eighteenth century not only was the sailing time from England reduced to about six weeks—one ship made the voyage from London to Boston in twenty-four days—but, more important, the number of ships and passengers increased greatly, so that the chances of importation were greatly multiplied. Chance importation alone, therefore, could account for the increase in number of eighteenth-century epidemics. But to explain why the increase was orderly it is necessary to consider changes in population density. During all of the seventeenth and most of the eighteenth century the population was so scattered over such a wide area that after any one widespread epidemic no second one of like extent could occur, even had measles been imported, until there had been a renewal of a concentrated group of susceptible persons, because after any large epidemic immune persons far outnumbered the nonimmune. This explains the failure of widespread epidemics to develop from the small local ones in Hingham in 1722 and in Falmouth in 1736. It can be assumed that most adults who crossed the ocean were immune because epidemics abroad were fairly frequent; hence the chief, if not the only, factor which caused the balance between immunes and nonimmunes to become reversed was the constant addition of new crops of susceptible children. Given a constant birth rate, a steady growth in population density obviously produced a more and more rapid renewal of concentrated groups of nonimmune children, a fact which explains the orderly increase in frequency of epidemics.
Today we are measles self-sufficient. That is to say, we are fully capable of breeding our own measles and no longer dependent on Europe for our epidemics simply because the population density is so great, and consequently the annual crops of susceptible children so large, that measles has become capable of propagating itself and so never entirely disappears from our large cities. In thinly populated, isolated country towns, however, conditions remain similar, so far as measles is concerned, to those of the eighteenth century, and one can still reach old age without experiencing the disease. It may therefore be concluded that there is a certain population density at which measles becomes capable of propagating itself. It is difficult to say exactly when that density was reached in this country, but it was probably before the middle of the nineteenth century, when the largest cities began to report measles cases every year.
Just as interesting as the change in epidemic frequency is the change in severity between early epidemics and those of today. There was certainly justification for alarm in the early days. No significant case fatality rates are available35 because it is impossible to estimate the ratio of deaths to the numbers who were sick; but the death rates, or number of deaths in relation to population, seem appalling when compared with the present rate. The fact that measles has changed from a disease of all age groups to a disease of childhood may account in part for this apparent reduction in severity, because it is believed that children withstand the disease better than adults. But this cannot be the whole explanation since many adults were involved in the epidemics of 1657, 1729 and 1759, which were supposed, at least in Boston, to have been relatively mild.
Another possibility is that different epidemics were caused by different strains of measles virus, some more deadly than others. Aside from the fact that there is at present no evidence of more than one strain of measles virus, one may nevertheless surmise that the mild epidemic of 1657 was caused by a different strain from the one that caused the severe epidemic of 1713. One might, however, start with the premise that each epidemic was caused by a single strain because it seems unlikely that two or more strains were imported in one year, say 1687, when not even one strain was imported in the other fifty-four years between 1687 and 1713. But very few, if any, epidemics were either uniformly mild or uniformly severe. In every one about which enough facts are known to warrant definite conclusions there were areas where the death rate was high and others where it was low. Hence a possible variation in strains cannot be more than a partial answer.
The one outstanding factor that varied from time to time and from town to town was the incidence of other serious diseases. The supposedly severe epidemic in Quebec during 1687 was complicated by another disease called “spotted fever.” It is possible that the severe epidemic in Boston during 1713–1714 may have been caused by two diseases.36 The 1729 epidemic in New York may have been severe only because of the prevalence of the disease called “pain in the side.” Throat distemper raged in parts of New England during 1739. Dysentery was said to have accompanied measles in Connecticut during 1758; and many children had “flux” and measles in Williamsburg during 1773. The five deaths during the Middletown epidemic of 1783 were attributed to either “Measles & Chincough” or “Measles and Dysentery.”37 Dr. Benjamin Waterhouse wrote in 1783: “In some seasons the Measles are very malignant; at present as far as I have seen, they are mild, regular, and unmixed—yet I am not without my suspicions that pulmonary disorders, and gradual wastings will attend not a few of the more infirm.” Since tuberculosis was exceedingly common throughout the eighteenth century it is more than probable that measles was many times only the final blow. It is therefore necessary, in any explanation of the high mortality of early measles epidemics, to take into consideration the presence of other diseases.
Diphtheria
In colonial records one looks for diphtheria under the name of cynanche, squinancy, quinsy, angina, canker, bladders, rattles, hives, throat ail, or throat distemper. It is said that the first epidemic occurred about 1659. According to Cotton Mather, it was during December, 1659, that the Reverend Samuel Danforth lost three children within a fortnight from “Bladders in the Windpipe,” which could have been laryngeal diphtheria. Scattered references to probable sporadic cases or local epidemics can be found particularly in Connecticut and Massachusetts between 1712 and 1735. John Walton’s Essay on Fevers, the Rattles & Canker (Boston, 1732) was the earliest American article on diphtheria, but it was, unfortunately, only a pompous display of useless theories.
The most frightful epidemic of any childhood disease in American history began in 1735.38 It appeared suddenly in Kingston, New Hampshire, during May, 1735, and gradually spread northward along the coast of Maine and southward into Essex County, Massachusetts. For some strange reason Boston and most of the surrounding towns were not involved to any great extent; for the epidemic, as it approached Boston, turned to the west and southwest and eventually fused with a similar epidemic which had started in New Jersey about the same time and had spread to the northeast.
This epidemic seems to have been most severe in the small frontier towns. In Kingston the first forty cases were fatal, and within a few months about half of all the children died. More than half of all the children of Haverhill died. In Hampton Falls one-sixth, and in Byfield and Rowley one-eighth of the population died. In New Hampshire there were at least fifteen hundred deaths out of an estimated population of less than twenty thousand. In Essex County alone there were fourteen hundred deaths. Altogether this so-called “throat distemper” caused five thousand deaths in New England within the first five years.
Over and over again it was called a “new” disease, for no one then alive could recall having seen the like of it before. An analysis of nearly one thousand fatal cases in New Hampshire during 1735–1736, however, reveals that over ninety-five percent were under twenty years of age. Consequently most adults must have been immune; hence, in spite of contemporary opinion, it could not have been a “new” disease.
The most characteristic feature of this epidemic was the occurrence of multiple deaths in families. There were at least six instances of eight deaths at a time, as in the family of John and Marcy Wilson of Andover:
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
In Hampton Falls one family lost seven children, two families lost six, two lost five, six lost four, and about fourteen families lost three apiece. It appears that certain families, such as the Boynton, Cressey, How, Lock, Moulton, and Pool families, were particularly susceptible, many branches of these families losing two to five, sometimes all, of their children. Children of ministers and physicians also figure prominently in the mortality lists, probably because the disease was carried home by their fathers, few suspecting that it was contagious. Death generally occurred within a week, frequently within a few hours when the disease settled in the larynx. As a rule the disease spread slowly from one town to the next at the rate of about ten miles a month, but occasionally six months elapsed before it spread to another town. Sometimes it appeared in isolated distant towns when there were no apparent contacts, and it would also seem to disappear from a town, only to return the following year. By 1740 the Connecticut phase of the epidemic which had started in Stamford had spread diagonally across that colony to Killingly; and the New Hampshire phase, though still causing multiple deaths in Newbury, Concord, Lexington, Lynn, Sudbury,39 and other towns north and west of Boston, was most active in towns near Worcester. Ebenezer Parkman, making notes in his diary during that “melancholy Time,” recorded days of fasting and prayer in Westborough, Southborough, Marlborough, Hopkinton, and Grafton. Measles was still prevalent in this region during the summer of 1740; and during the following spring, yet another disease complicated the epidemic at Sutton. The Reverend David Hall recorded in his diary for April 6, 1741: “Nineteen persons have died with the long fever: many more of the throat distemper; no less than five in one Family God’s hand is upon old and young, especially upon my People.”40 By the end of 1741 the epidemic had spread over nearly all the settled regions of New England.
A rare broadside published during one of the diphtheria epidemics (? 1736)
Reproduced by courtesy of the late Dr. Josiah C. Trent
After the initial outbreak in a town the disease would quiet down for a while but, unlike measles, it would never entirely disappear. In many towns one can find multiple deaths from throat distemper for two or three years following an epidemic peak, but usually the disease would recede more and more to a period of comparative calm, only to be followed by another outbreak. At first sight no general pattern is discernible in these subsequent waves, and a mere list of New England epidemics after 1741 appears to be a meaningless array of dates. But if a certain group of towns is selected for study, it looks as if the disease kept reappearing at intervals of seven to ten years. Thus in New Hampshire, Stratham and Greenland were revisited in 1742, Newmarket in 1743, Kingston and Exeter in 1744, and Hampton in 1745.41 A third epidemic wave swept over this same area, involving Exeter, Stratham, and Rye in 1753, Hampton and Kingston in 1754, and East Kingston in 1755.42 Again, these subsequent waves, unlike those of measles, were not dependent on fresh importation, because it is doubtful if New Hampshire was free from the disease at any time between them. Nor does it appear that the disease spread directly from one town to the next, as it seemed to do in the first severe outbreak. Therefore, particularly in view of the slight variation in dates, it is surmised that these subsequent epidemics were chiefly dependent on new crops of susceptible children. Apparently it took seven to ten years, depending somewhat on the number of births, for nonimmune subjects to become numerous enough for an epidemic to occur.
In Massachusetts, to find any sort of pattern in the numerous epidemics, it is also necessary to study towns of a certain area. In the northeastern part of the province, very little information is found about the disease after 1741 until the cold months of 1747 and 1748, when there were numerous multiple deaths.43 The cause of these deaths still remains unknown; but they were probably due to throat distemper, since that disease was the cause of most of the deaths during the epidemic in Bedford, Billerica, Byfield, Chelmsford, Tewksbury, and Wakefield during 1749–1750.44 On the whole, these epidemics were less severe than those in this region during the previous decade; but one can hardly call them mild when there were numerous instances of three or four deaths in a family. It appears, however, that epidemics varied in severity in different towns, depending somewhat on the extent of previous damage. When one epidemic was widespread enough to cause a large number of deaths, the following one was usually less destructive. The available Tewksbury records show no large epidemics after the one in 1749, although a few deaths from “canker,” “quinsy,” or “throat distemper” occurred during many of the next fifty years. On the other hand, in other towns of this area epidemics continued to occur in waves. There was another outbreak during the years 1753–1756, particularly in Byfield, Chelmsford, and Concord;45 and still another from 1761 to 1765, particularly in Andover, Byfield, Boxford, Bradford, Haverhill, and Groton.46 It was said that the Haverhill epidemic “was in a milder form [than in 1736], or was better understood, and but few died.” Thereafter epidemics in this region became more and more rare. There were a few multiple deaths from “canker” in Middleton during 1769;47 and more from some unidentified disease, probably throat distemper, in many towns during the cold months of 1778. There were also many single deaths from “canker” and “sore throat” here and there almost every year, and particularly during the scarlet fever years of 1784 and 1795, but there were no epidemics at all comparable to the earlier ones.
In southeastern Massachusetts the disease was most erratic in its progress, or so it seems from the records now available. Multiple deaths began to occur in Bridgewater about December, 1746, and were followed during 1747–1749 by others in East Bridgewater, Kingston, Scituate, Cohasset, Braintree and Halifax.48 It was said of Kingston:
Jan. 7. 1747, 8. The Sickness in this Town remains exceeding bad; but here has been one Instance the like of which has not been known in the Memory of Man, viz. Mr. Thomas Cushman of this Town had jive Children of his own and another related to him in his House, four of his own Children died about a Week ago within the Space of eight Hours, of the Throat-Distemper, and this Week the other two Children died, and the Family left childless. About 30 have died in this small Town in a few Months past, and three of them grown in years, the rest Children.49
After a lull of about a year, that is, during 1751–1752, some terrible epidemics reappeared in this same area but in different towns—Abington, Attleborough, Hanover, and Weymouth. Twelve percent of the population, or 150 persons, mostly children, died in Weymouth during “The Throat Distemper Year” of 1751.50 The Colson family lost four children in January, 1752, and three more from “throat ail” in 1760.51 About eighty children died in Hingham.
Though the disease in eastern Massachusetts seems to have quieted down considerably after the seventeen-sixties, it continued its periodic outbreaks in the small towns of the north-central section. An epidemic in Westminster in 1764 was followed by another in Athol in 1776 and another more severe one in Princeton and surrounding towns in Worcester County during 1786. The newspapers called the disease “the most fatal one, to children especially, of any known in this country.” The next severe one had its center in Royalston, where fifty-seven children and nine adults succumbed in 1795. At least three families lost five apiece. That year five in one family died in Rutland also.52
My records of other sections of Massachusetts are at present so incomplete that no conclusions concerning the behavior of the disease over a long period of time seem justified. Some of these are newspaper accounts of multiple deaths in one family, and efforts to find an epidemic have been fruitless. On the other hand, there were many fairly severe epidemics accompanied by multiple deaths which were not even mentioned in the newspapers. One notable exception was the frightful epidemic which raged in Oxford between 1767 and 1770.53 It caused the deaths of one hundred and forty-four persons, mostly children two to fourteen years of age, which was twelve percent of the population. Two families each lost eight children. One possible explanation for this high mortality is that the disease seems to have been relatively rare in Oxford after the epidemic of 1740–1743.
In certain areas of Connecticut the disease also seems to have occurred in waves, but there is little justification for enumerating twenty or more different outbreaks until the history of the disease in that colony is more complete. Only scattered references to epidemics in other colonies are available at the present time.
In one respect diphtheria differed from any other disease. In such areas as northeastern Massachusetts and New Hampshire, where for a period of about forty years it had kept recurring in epidemic waves, after the Revolution it gradually caused fewer and fewer deaths in spite of a great increase of population. It never entirely disappeared, for one can find here and there single deaths and even an occasional small epidemic attributed to “canker,” “quinsy,” or “throat distemper.” Yet not only did the total deaths from this disease fail to increase with the growth of towns, but the incidence of multiple deaths also fell off appreciably. Instances of five or more deaths in a family, so characteristic of the early epidemics, are noticeably absent after 1780. Even four deaths in a family are difficult to find. Scarlet fever was prevalent during most of this period and was frequently confused with diphtheria; but even allowing for difficulties in interpretation and attributing the worst scarlet fever epidemics to diphtheria, one still cannot find any epidemics to equal those between 1735 and 1770. It is also significant that Dr. Ebenezer Beardsley (1786), Dr. Hall Jackson (1786), and Dr. Edward Holyoke (1797) all spoke of old-fashioned throat distemper as a disease that had not been seen for years; and Jeremy Belknap’s figures for New Hampshire show a decided decrease in the incidence of the disease as the century closed. Since terrible epidemics were to return to these same areas later in the nineteenth century it appears that the recurring epidemic waves which began so explosively in 1735 were in turn only a part of a greater cycle in the age-old chronicle of diphtheria. These great cycles were certainly independent of any methods of treatment or prevention, and apparently independent of quantitative changes in population. Should further studies of other areas reveal similar great cycles in diphtheria incidence, one should be better able to understand the curious natural history of this terrible disease.
More facts are needed to determine whether these great cycles were caused by changes in the disease itself or by changes in population immunity. From the facts now available it appears that the population had gradually become more resistant possibly because a large proportion of the children in the more susceptible families had failed to survive the repeated epidemics. A change in the virulence of the causative organism hardly explains the fact that during the last quarter of the eighteenth century, when the disease was on the wane in the old established towns of eastern Massachusetts and New Hampshire, malignant epidemics began to appear in the small towns of Maine, Vermont, western Massachusetts, Ohio, and Kentucky—towns nearer to the periphery of a rapidly expanding civilization, and towns with populations which had not been immunized by previous epidemics.
Scarlet Fever
Brief references to an epidemic of scarlet fever in Boston between September and December, 1702, can be found in the diaries of John Marshall and Cotton Mather.54 Medical historians usually disregard this epidemic, chiefly because Noah Webster, the authority on early American epidemics, accepted the opinion of William Douglass, who, some fifty years after the event, said that it was not scarlet fever at all but hemorrhagic smallpox.55 Back in 1702, however, both Marshall and Mather apparently thought that they were dealing with two separate diseases; and further proof that real scarlet fever was present about that time is contained in Mather’s letter to Samuel Penhallow, which was written in December, 1704:
. . . My daughter Katy, is yesterday taken Dangerously and Violently sick of the Scarlet Feavour; and we are with much Care and Fear waiting the event of the Sickness. My next Daughter, was taken ill of the same Distemper, at the same Time. And my only Son, who has been longer down is yett very ill of it. My Family is on these Accounts very much under the fatherly Chastisements of God. God make me and mine Gainers by his Chastising Dispensations: and preserve our Neighbourhood, from the spreading of a Calamity, which I doubt is becoming Epidemical.56
This could not have been hemorrhagic smallpox because these children had smallpox in 1702.
The next large epidemic of which I am aware began in 1735, but it was then described by the doctors as a “new” disease. Both William Douglass, in his classic The Practical History of a New Epidemical Eruptive Miliary Fever (Boston, 1736),57 and Jonathan Dickinson, in his Observations On that terrible Disease Vulgarly Called the Throat-Distemper (Boston, 1740), described a disease which they claimed was not only new but also distinguishable from scarlet fever, yet they mentioned signs, symptoms, and complications which indicate that it must have been the same disease that is now called scarlet fever.
There is considerable information available about the great scarlet fever epidemic in Boston during 1735–1736.58 It first appeared in August, 1735, among a small group of children of the North End, and by September it had spread to several other parts of the town. During the winter it continued to spread until it reached its peak in March and by July it was “almost over.” It was estimated that there were about four thousand cases in a population of sixteen thousand. Douglass noted that it was predominantly a disease of childhood, which means that adults were immune from previous exposure. Thus it could not have been a “new” disease. Though he mentioned a few signs and symptoms which are seen only in diphtheria, there can be no question but that he was dealing primarily with scarlet fever, for he enumerated practically all the signs and symptoms of that disease. He called attention to the intense prostration, delirium, swollen glands, and desquamation. He even mentioned the strawberry tongue, rheumatic pains in the neck, wrists, and ankles; and, alone among early writers on this disease, he noted some cases with bloody urine. His cases varied in severity from benign to malignant, a few of the latter dying within three days. In some there were extensive hemorrhages, and there were some with purpuric spots on the skin; but these cases apparently were rare. During 1736 the disease appeared in Marblehead, Ipswich, and Haverhill, but no detailed accounts of these epidemics are available.
Scarlet fever today is, by and large, a mild to moderately severe disease with a case fatality rate of less than one percent; but one needs to go back only one generation to find that it used to be severe. Hence it is frequently stated that until very recent times scarlet fever has always been a severe disease. That is an unwarranted conclusion because the one important fact revealed by a study of the 1735–1736 epidemic is that scarlet fever at that time was also comparatively mild. Douglass computed that there were 114 deaths out of 4,000 cases—a case fatality rate of 2.8 percent; and another independent observer of this same epidemic said that fatalities were less than one in sixty—a rate of 1.7 percent. “Very few died” in the Marblehead epidemic, nor was the disease very alarming during another epidemic in Guilford, Connecticut, during 1740.
The Boston doctors, fully aware of the relative mildness of their epidemic, arrived at some astonishing conclusions which had lasting effects on American medicine. It will be recalled that a malignant diphtheria epidemic started in New Hampshire in 1735 just a few months before the outbreak of the Boston scarlet fever. Having had little or no experience with diphtheria, the doctors unanimously declared that it was caused by “bad air” and was definitely not contagious. Then, after observing that these epidemics were similar in that children were the victims and sore throat was the chief complaint, they decided that both were caused by one and the same disease. To explain why it was so alarmingly fatal in New Hampshire and so surprisingly mild in Boston, they concluded that the atmosphere was more healthy in Boston, their patients were physically superior, and, last but by no means least, Boston doctors were better doctors. Their theory was that the disease was naturally accompanied by a rash, and a physician had only to prescribe the kind of treatment which would allow the “morbifick matter” within the body to reach the surface, evaporate through the pores, and thereby produce the rash. The rash, therefore, was the proof of successful treatment. In New Hampshire very few patients had rashes, and fatalities were about sixty percent; in Boston nearly every patient had a “laudable and salutary” rash, and fatalities were about two percent. It was a wonderful and comforting theory—for the Boston doctors.
This theory that scarlet fever (or “canker rash”) was fundamentally the same disease as diphtheria (or “canker”), though originally founded on false conclusions and conceit, nevertheless makes it difficult to evaluate the severity of these diseases, and particularly scarlet fever, in subsequent colonial records. Not only was no attempt made to differentiate them, but also the two diseases so frequently coexisted that it is difficult to find many epidemics of unquestionable scarlet fever for study. But with the exception of the easily frightened Cotton Mather, who said that scarlet fever was dreadful, dangerous, violent, and mortal (perhaps it was in 1702–1704), all other early eighteenth-century sources reveal that it was not a very severe disease. Besides the convincing records of the Massachusetts epidemic of 1735–1736, Cadwallader Colden of New York intimated that it was relatively mild; and Jonathan Dickinson said that in New Jersey it was “not very dangerous: I have seldom seen any die with it, unless by a sudden Looseness, that calls in the Eruptions; or by some very irregular Treatment.”59 Parson Smith of Falmouth, mentioning an epidemic of “the Rash” in April, 1753, remarked: “Thank God, it is in so few instances mortal.”60
There are not many records of even isolated cases of scarlet fever between 1753 and 1770, but during the last three decades of the century the disease apparently became increasingly common, and there are not only records of numerous epidemics but also a few very good clinical descriptions. The first-of these was Lionel Chalmers’s account of an epidemic in Georgia and South Carolina during 1770.61 Chalmers described what seemed to him an alarming disease with chills, fever, vomiting, delirium, sore throat, and scarlet rash, followed by desquamation and painful swollen extremities; he added, however, that most of his patients recovered. He had not seen any similar cases for over eighteen years. This could not have been a new disease in South Carolina because most of his patients were under fifteen years of age, and, of the few adults who were sick, nearly all had sore throats without eruptions—an indication of some degree of immunity from previous exposure.
The first good evidence of severe scarlet fever in New England is the newspaper account of a Duxbury epidemic during the spring of 1771. It is worth noting that this, too, was primarily a childhood disease; which is indirect evidence that scarlet fever had been more or less prevalent in New England from 1753 to 1771, even though very few records have been found.
Duxboro, July 5, 1771
A very malignant putrid Fever has, for some Time past, much prevailed in this Town; about 150 Persons, chiefly Children, having had it in the Course of a few Months; to a considerable Proportion of whom it has proved fatal. More especially of late its Malignity has very much increased. And in one Family in particular, (Mr. Benjamin Wadsworth’s) five Children out of Six have died of it in the short Space of a Week; the only one surviving being now dangerously sick.—This Fever seems to differ from what has been usually called the Scarlet Fever only in Point of Malignity; the Appearances in those who have it favourably being in all Respects the same. It is remarkable that though it has made its Appearance in every Part of this Town, scarce a Family or Person in any of the neighbouring Towns have as yet been visited with it.62
The deaths of five Wadsworth and three Soule children in Duxbury during May and June, 1771, and of three Fuller children from “canker rash” in East Haven, Connecticut, during 177363 suggest a malignant type of scarlet fever, one capable of causing multiple deaths. But one must be cautious in accepting multiple deaths alone as evidence of severity because diphtheria, the most common cause of multiple deaths, was still breaking out here and there, and hence these children may have had both diseases. Moreover, the report states that those who had it “favourably” had a disease just like scarlet fever. This makes one wonder whether those who had it unfavorably may not have had something else. If one assumes, however, that scarlet fever was the only disease in Duxbury, it seems that it had been mild up to 1771, when it suddenly appeared “very malignant.” Even so, there is good evidence that it was still less fatal than diphtheria. Jacob Ogden, for instance, in his account of “Malignant Sore Throat” as it appeared in the vicinity of Jamaica, New York, in 1774, had this to say about scarlet fever:
Sometimes, especially near the Equinoxes, the Disease is attended with Eruptions, commonly called a Rash. In this Species, the Symptoms previous to the Eruptions are generally more violent, often attended with a burning Fever, great Anxiety, a Diarrhœa or Flux, Delirium, &c. until the Eruptions are fully out.—This is not so dangerous as the former, especially if the Efflorescence or Eruptions appear before the third Day.64
There was an epidemic in Dighton, Massachusetts, about 1773; another in Philadelphia during 1774; and there are a few scattered references to cases or deaths in New England during 1775 and 1776. There were also epidemics among Montgomery’s and Arnold’s troops at Quebec in 1776, but the accounts throw very little light on the nature of the disease.65
The lack of references to scarlet fever between 1776 and 1783 does not necessarily mean that the disease was absent or even rare because, as has been shown, most scarlet-fever-free periods were followed by epidemics in which adults were usually immune. But if the disease was present during this period, at least it can be said that it did not cause much concern. Between 1783 and 1791, however, the marked increase in both lay and medical records concerning scarlet fever suggests that it was exceedingly common; and there was at least one sizable epidemic in every state from Maine to Maryland. A 1786 newspaper stated that “the throat-disease . . . for more than two years past has prevailed in the Eastern states, and proved fatal to vast numbers of children.”66 This could not have been diphtheria entirely, because the item goes on to say that in the Attleborough and Rehoboth epidemics none of the patients died. The Sutton vital records reveal a death from “Canker Rash” in 1784, 1785, and 1786. Elsewhere there were epidemics during two successive winters. In places where adequate records were kept it appears that the disease was present for a good part of the time. In Philadelphia, for example, there were numerous cases almost every year from 1783 to 1791.67 In Vermont, too, from 1783 to 1790, the disease was “very prevalent almost the whole time, but in different places in different periods of the term.”68
It is difficult to draw any blanket conclusion about the severity of scarlet fever during this period, for the records vary considerably, depending upon the place and time. Noah Webster, in one article, stated that during 1784 scarlet fever “fell lightly” on the western part of Connecticut “but was more severe in the eastern towns, and in Massachusetts, New Hampshire and Rhode Island.” In another article he stated that the disease “was not severe in general and many towns wholly escaped its attacks.”69
Thus, in the absence of any figures or definitely reliable statements, one must consult the clinical accounts to obtain some idea of the nature of the disease. In his description of the epidemic which started in Philadelphia and later spread to New Jersey, New York, Delaware, and Maryland (1783–1784), Benjamin Rush mentioned such complications as middle-ear disease, swelling behind the ears (mastoiditis?), troublesome sores on the ends of the fingers (paronychia?), rheumatism, and dropsy of the limbs, abdomen, and thorax, all of which together indicate a fairly severe variety of the disease. In fact, with candid lack of modesty, Rush claimed that when his method of treatment was not followed, the disease was often fatal. Dr. Edward A. Holyoke, in his bill of mortality for Salem (1783),70 listed six deaths from scarlet fever, four of them from a complicating “Anasarca,” which is good evidence that the disease was sometimes severe in New England too. No details are at present available for the epidemics in Providence, Newport (1783–1784), Lyme, Middletown, Charleston (1784), or Sterling (1786).71 But Dr. Gallup said that between 1787 and 1790 the disease was “very fatal” in many places in Vermont and that it “severely affected the inhabitants of the western part of New Hampshire.”
It is more than probable that some of the deaths attributed to scarlet fever during this period should really be attributed to a combination of diseases. Hall Jackson’s account of an epidemic that extended from northern Massachusetts to southern Maine during 1784–1785 is conclusive proof that scarlet fever epidemics were still complicated by diphtheria.72 Though one can read a few cases of diphtheria into nearly all eighteenth-century accounts of scarlet fever, this one in particular is most confusing unless both diseases are borne in mind. Jackson was undoubtedly dealing primarily with a fairly severe scarlet fever, but his clear, concise descriptions of palatal paralysis and fatal laryngitis prove that diphtheria caused some of the deaths because these complications never occur in scarlet fever. From a purely scientific standpoint his account is therefore valueless, but he nevertheless made some interesting observations. He noted, for instance, that many women died from puerperal fever just before the epidemic began. He called his epidemic “Putrid Malignant Sore-Throat” because the sloughs in the throat caused a putrid odor to the breath. He distinguished this from old-fashioned “throat distemper” on the basis of a lower fatality rate, but naturally an epidemic of both scarlet fever and diphtheria would have a lower fatality rate than an epidemic of diphtheria alone. He also distinguished his epidemic from the disease “commonly called the Scarlet Fever” (this, by the way, is proof in itself that scarlet fever was common before 1784) on the ground that “an efflorescence always appears in the Scarlet Fever,” and many of his patients did not have rashes, and some had had scarlet fever previously. Jackson was, on the whole, correct in distinguishing diphtheria from scarlet fever on the basis of a rash, but he did not realize that a second attack of scarlet fever, particularly in an adult who had had the disease in childhood, would not produce a rash.
William Baylies’s description of an epidemic of “Ulcerated Sore Throat” in Dighton, Massachusetts, during 1785 and 1786,73 though not startling, is one of the best accounts of scarlet fever during this period, especially since he did not include any purely diphtheritic signs or symptoms. Though he was unable to prove it in all instances, he maintained, as did Hall Jackson, that the disease was “evidently contagious.” It seems a pity that this opinion did not carry more weight, for had it been accepted, American medicine could have been spared a lot of foolish arguments later on. Baylies included a few brief but choice descriptions of various complications, including suppurating glands, acute rheumatism, and universal edema. He was the first American writer, so far as I know, to associate this universal dropsy with the urinary system: “At this time they made but little water.” He did not call the disease “scarlet fever,” chiefly, I suppose, because half of the afflicted adults did not have rashes. The article is useful in interpreting subsequent records because it shows that “ulcerated sore throat” was no longer reserved for diphtheria but was even applied to uncomplicated scarlet fever.
In contrast to the evidence indicating that scarlet fever was a severe disease are the Attleborough and Rehoboth records of epidemics without deaths, and also the Philadelphia records of 1791, which say that the disease “seldom proved fatal.”74 It may be significant also that so far no instances of multiple deaths from scarlet fever have been found for the period 1783 to 1791. The most one can say is that in general the clinical accounts show a fairly severe variety of the disease at times, but apparently the average case fatality rates were not very alarming.
A study of the records from 1792 to 1798 shows a still greater increase in both prevalence and severity, or at least many more notes pointing in this direction can be found. But even in spite of more detailed descriptions, the confusion that surrounds all eighteenth-century accounts of scarlet fever becomes more confounded as the century closes. By this time Benjamin Rush, the most influential teacher in this country, had succeeded in reviving Sydenham’s doctrine of “epidemic constitutions” and particularly emphasized that “no two contagious fevers of unequal force can exist long together in the same place.” Rush described epidemics of scarlet fever and chicken pox as though they had a common cause. Naturally, therefore, lesser men were ready to believe that such superficially similar diseases as diphtheria and scarlet fever must have been related. The complex and inaccurate classification of diseases by Professor William Cullen of Glasgow was also widely respected in this country. It remained only for Noah Webster to group all sorts of diseases together in order to show that all epidemics could be traced to atmospheric disturbances, earthquakes, or volcanoes. This period could be called the dissertation decade of medical history; and since scarlet fever received its fair share of attention from students who were candidates for degrees, a few facts on the character and epidemiology of the disease are revealed. But the emphasis was mostly on theory, and students debated whether the disease was “inflammatory,” requiring antiphlogistic treatment such as bleeding and purging, or whether it was “putrid,” requiring antiseptic treatment such as tonics and stimulants, particularly quinine. Whether the disease was directly contagious from person to person or caused by “contaminated air” was still a serious unsolved question. Three types of the disease were recognized. First was the relatively mild scarlatina simplex, a few writers maintaining that not even a sore throat was necessary in this variety. This type was seen in every epidemic.75 Apparently the most common type was the so-called scarlatina anginosa, or those cases with white or ash-colored ulcers in the throat. Also mentioned by most authors was the fulminating scarlatina maligna, characterized by intense prostration, sustained high fever, almost constant delirium, excessive vomiting or diarrhea or both, sometimes purpuric spots or profuse hemorrhages, generally causing death within the first week. These were the cases that were confused with diphtheria because of the extensive membrane in the throat and because a few patients failed to show a rash. There was no sharp line of demarcation between the various types; consequently one finds scarlatina maligna, angina maligna, cynanche maligna, and “canker rash” used as synonymous terms. Indeed, Matthias H. Williamson, who wrote one of the best articles on the disease,76 refused to differentiate the types because, as he said, no one could do it in practice, and besides there were already enough diseases! All told, the resulting confusion makes contemporaneous material difficult to interpret, and only by disregarding terminology and paying strict attention to clinical descriptions and case fatality rates can one make sense out of the accounts of various epidemics.
Noah Webster, probably influenced by an account of a small epidemic in Bethlehem, Connecticut, where no deaths occurred out of seven or eight cases, described the scarlet fever of 1792 as “mild”; but Willett Taylor’s account of an epidemic in New York77 reveals a moderately severe disease. During the following winter, and particularly during the spring of 1793, malignant scarlet fever was reported in New England, New York, and Philadelphia. According to Rush,78 the Philadelphia epidemic from February to August reached its peak in July “with symptoms of great violence.” Six patients died in one parish in Morristown, New Jersey.79 In New York City there was “great mortality,” and in some cases at Red Hook “the paroxysms invaded the patient in the form of madness.”80 Connecticut records vary considerably. There were no deaths during an epidemic in Hartford from April to May, nor any among “several cases of ulcerous sore throat” in New Haven. But the disease was said to have been “very mortal” at New Fairfield, and other deaths occurred at Branford, Fairfield, Middletown, Preston, and Stonington.81 The few available details concerning the disease in Massachusetts and Vermont are insignificant.
It was said that during 1794 scarlet fever raged “all over the country,” but my material concerns only Connecticut,82 where there were epidemics in Bethlehem, Branford, Bolton, Cheshire, East Haven, Hamden, Hartford, Lebanon, Preston, and Woodbridge. The epidemic in New Haven between January and July seems to have caused the most alarm. Ezra Stiles speaks of the fear that spread among the students at Yale when a freshman died after two days of “Angina Ulcerosa”; and in April the faculty finally yielded to the demands of the students and voted to close the college. By April 10 a committee of physicians, in a statement published to offset the exaggerated reports that had spread throughout the state, said that out of 290 cases “only eight have died. The malignancy of the disease has abated, and its symptoms appear comparatively mild.” By July, however, there was a different story because forty-three had died of “malignant Scarlet Fever.” After the epidemic was over, it was found that 52 died out of 750 cases—a case fatality rate of 6.9 percent. A broadside published in October described the disease as “very mortal.”
These New Haven figures make it appear that scarlet fever in Connecticut during 1794 was a rather severe disease; but Dr. Thaddeus Clark of Lebanon, writing of the disease in eastern Connecticut, said: “It is well known, that the Scarlatina Anginosa, in these parts, in the spring, summer and autumn of 1794 . . . was generally of the mild, more simple inflammatory kind.” He quoted other doctors as saying: “a Doctor is a fool that loses patients in the Canker Rash.”83 This discrepancy in the accounts of the same disease in the same state in the same year is a good example of the marked variations of the disease or of a difference in diagnostic standards. The latter is supported by the Bethlehem records, which say that “Many who now [1794] had the disorder, had had it in 1793”; and the same account mentions diphtheria (cynanche trachealis) in 1792. Therefore one must at least consider the possibility that some diphtheria was present, particularly in those regions where the case fatality rates were high.
During 1795 there were scarlet fever deaths in at least sixteen Massachusetts towns.84 The Boston epidemic began in the spring. At least seventeen died in Beverly, and eleven in Topsfield. In Sterling between March 1, 1795, and April 18, 1796, there were 8 deaths out of 150 cases, or a case fatality rate of 5.3 percent. Twenty-one died in Marblehead during 1796.85
Beginning early in 1796 and continuing through 1797, the disease seems to have been severe in the small towns of Vermont. Dr. Gallup described epidemics causing 20 to 25 deaths in towns of 150 families. It was mostly confined to children, though it also attacked some old people who had had it during childhood. There seems little doubt that the case fatality rate was high, but, as in so many other accounts, here also are some indications of diphtheria. Gallup said that some of the cases terminated in “difficult respiration” and “some cases had no vestige of eruption.”
During 1796 and 1797 the disease was also prevalent in New Hampshire, particularly at Portsmouth and Hanover. During the winter of 1797–1798 there were cases reported from nearly every town in Cumberland County, Maine, and it was “mortal in many instances.” Dr. Jeremiah Barker of Portland, Maine, lost two out of fifty cases, or a case fatality rate of 4 percent.86
In spite of diverse and apparently contradictory material concerning scarlet fever in the eighteenth century, certain broad generalizations can be made. Epidemics appear to have occurred in waves, with long interim periods during which little was said about the disease. At each reappearance, however, adults were generally immune, showing that the disease had at no time entirely disappeared, and in support of this conclusion one finds in almost every account some such statement as “commonly called a scarlet fever,” as if every layman had been long familiar with it. There are three reasons for supposing that as the century progressed a malignant type of scarlet fever appeared with increasing frequency. The earliest available statistics show a case fatality rate of about two percent, whereas the last statistics show a rate of about six percent. William Douglass in 1736 described some fulminating cases, but in view of his statistics and comments they seem to have been rare, whereas these cases were more frequently described in the closing decade. It is in the last decade, too, that one finds most of the multiple deaths attributed to “canker rash.” I have found sixteen instances of two deaths in a family and three instances of three deaths in a family. This is a far cry from the wholesale instances of multiple deaths during diphtheria epidemics, yet it is additional evidence of a more virulent type of scarlet fever. But the most important fact of all is that in dealing with scarlet fever all clinical accounts and all statistics should be somewhat discounted because of the confusion with diphtheria. To separate these two diseases now, when eighteenth-century doctors themselves made no attempt to separate them, is at best a difficult task. At times it is impossible.
Whooping Cough
The name “chin cough,” commonly used for this disease in the seventeenth and eighteenth centuries, was said to have been derived from either kind (“child”) or kink (“gasp”), but it is also possible that it came from quinta, the name used by Baillou in his original description of an epidemic (1578). Baillou did not know how the disease acquired that name, but possibly it had the same derivation as quinsy and was first used to mean a choking or a strangling cough.
In dealing with early fragmentary records it is well to bear in mind some possible errors in diagnosis. Other diseases sometimes passed for “chin cough.” During the great diphtheria epidemic in Haverhill (1736) one child was said to have died from “chin cough & throat distemper.” This case, in view of the tendency of inexperienced laymen to confuse whooping cough and croup, must be classified as doubtful. Similarly, the Reverend Thomas Smith maintained that both he and his wife had the disease in August, 1786, and again in December, 1787, which is hardly possible. On the other hand, whooping cough may have passed for other diseases. It is very likely that some epidemics of “very deep colds among children” were epidemics of real whooping cough, and though this is mere conjecture, the possibility may explain the paucity of early records.
Until one stops to consider that whooping cough, because of its hemorrhagic manifestations, was an alarming disease of childhood and its importation could have been easily controlled, it seems strange that references to epidemics before 1750 should be so scarce. The earliest were at Scituate and Barnstable and were occasions for “days of humiliation”:
June, 10. 1641 . . . for ye healing of a bloodye Coffe amonge children especially at Plimouth . . .
November 15, 1649 . . . God’s hand beeing uppon us by Sicknesses & disease many Children in the Bey dyeing bye the Chin cough & the pockes . . .
December 10, 1649. In regard of our owne particulars, very many amongst us beeing visitted with colds and coughes in a strange manner especially children theire coughing constraineing casting & bleeding att ye nose & mouth, & principally in regard of my self beeing brought very low by the cough & stitch in my left side, by reason whereof I was detained from Ministery seven weekes, but our God was intreated to shew mercye.87
There was a more extensive epidemic in 1659. The younger John Winthrop mentioned cases of “hoping cough” and “great hooping cough” in Hartford.88 “In this same month of December,” wrote John Hull, “the young children of this town [Boston], and sundry towns hereabout, were much afflicted with a very sore whooping-cough: some few died of it.”89 The records are a little confusing at this point, for the Reverend Samuel Danforth of Roxbury wrote: “9m & 10m [1659]. The Lord sent a general visitation of Children by coughs & colds, of wch my 3 children Sarah, Mary & Elisabeth Danforth died, all of ym within ye space of a fortnight.”90 These children probably did not die from whooping cough, however, for not only were multiple deaths exceedingly rare from this disease, but also there is some evidence of a diphtheria epidemic at this time, and Danforth may have failed to differentiate the two diseases.
I have no other records of whooping cough epidemics until 1738, an interval of nearly eighty years, which cannot be attributed to lack of records entirely, because in neither the Sewall nor the Mather diaries is whooping cough even mentioned. Thomas Robie jotted down in his medical notebook (1711–1715) some remedies “For Children’s Convulsive Cough . . . ye Hooping Cough of Children, wch is also termed ye Chin Cough,” but he merely copied Sydenham’s instructions and gave no evidence of first-hand experience.91
The next epidemics of which I am aware occurred in Connecticut and South Carolina. Joshua Hempstead entered in his diary on August 7, 1738: “an Infant of Samll Moseyers buried Died Last night with the Hooping Cough which is very Common in ye Town, it hath been in ye farms al Sumr.”92 There was another large epidemic in Charleston, South Carolina, in 1738,93 which may have had some relation to the New London epidemic, since both towns were important points of call in colonial coastwise traffic.
Another possible epidemic in New London during August, 1746, when a two-year-old child died “it is said from whooping cough,” and another “violent cough common among children” at Hanover, Massachusetts,94 during September, 1748, complete the record of epidemics before 1750. During the second half of the eighteenth century there appears to have been considerable variation in the prevalence of whooping cough, depending somewhat on the density of population and intercommunity traffic. In the best medical description of the disease Lionel Chalmers said that there had been only three epidemics in South Carolina previous to 1776. These were in 1738, 1759, and 1765. He also said that the disease had been “brought hither from other parts, its approach having always been heard of before it appeared amongst us.” In Philadelphia, however, the records of two Episcopal parishes comprising less than a tenth of the population show whooping cough deaths in twelve out of twenty-five years (1751–1775), with never more than two successive years without at least one death.95 The Presbyterian Church records of Morristown, New Jersey, show considerably fewer deaths: one in 1769, two in 1775, one in 1778, two in 1783, one in 1785, and four in 1791.96 In New England, although one finds very few references to epidemics in newspapers and only an occasional mention in diaries and letters, remedies for the disease appeared periodically in almanacs, and the vital records of various towns show that it was fairly common. With few exceptions all references fall during certain epidemic periods lasting one to three years and separated by fairly definite intervals: 1758–1759, 1765–1766, 1770–1771, 1777–1779, 1782–1783, 1786–1788, 1791–1792, and 1795–1796. Epidemics appear to have been most erratic in their progress. Widely separated towns were involved in the same year, while neighboring towns were involved in successive years. There was no significant seasonal variation, though epidemics were slightly more frequent during summer months.
While little was said about whooping cough in general terms, probably because it was mild in comparison with other epidemic diseases, a few statements reveal its serious nature. The New York Gazette and Weekly Mercury of December 25, 1769, describing an epidemic in Montreal, said that it was “at present extremely fatal to the children.” Chalmers called it a “dangerous and obstinate complaint”; and it was “very violent in many instances” in Philadelphia during 1791.97 However, the disease apparently seldom caused any great alarm, the Boston epidemic of 1765, for example, being mentioned in the newspapers only incidental to a note on the use of maple sugar—which was “as pleasant to the Taste as any other Sugar, and the Makers insist that it is medicinal, and very proper to give to Children for the Chin-Cough, at this Time very prevalent among us.”98 Moreover, it seldom caused multiple deaths. Aside from the questionable cases mentioned in the Danforth records (1659), the only other multiple deaths found so far were those of two of Joseph Tufts’ children in Medford during 1796.99 Also the case fatality rate was relatively low, for only one or two deaths occurred during most of the epidemics in small towns. But occasionally, particularly when epidemics coincided with epidemics of other diseases, the net result was startling. The worst epidemic so far encountered occurred in Salem during 1770, when there were thirty-seven “chin-cough” deaths in a population of about five thousand. Even the Salem newspapers had nothing to say about this epidemic except to print a remedy consisting of sweetened extract of colt’s foot (tussilago farfara), which had been found to “cure in two or three Days.” The bill of mortality for 1770, however, shows some “throat distemper” in the town, which may have contributed to this unusual mortality.100 Indeed, “canker” seems to have been a not infrequent complication throughout this period, for it was mentioned as a contributory cause of death in other towns such as East Bridgewater (1770), Sutton (1771), Middletown (1777), and Ipswich (1787).101 Thomas Smith wrote in his diary on October 25, 1786: “The whooping cough continues and with a dreadful cankerous disorder.” Whooping cough being a long-drawn-out affair, afflicted children were apt to pick up other contagious diseases before they had a chance to recover. Chalmers mentioned fatal diarrhea as a complication; and Holyoke listed seven deaths from “Chin cough combined with Dysentery and Cholera Dysenterica” during the Salem epidemic of 1782. In Middletown three children died from “Measles and Chin-Cough” during the epidemic of 1783.
There were at least three fatal cases of “Consumption which followed the Whooping Cough,” but in spite of the prevalence of tuberculosis this “consumption” may have meant any one of a number of complications. “Fever & Chincough,” which occurs frequently in the death records, undoubtedly included cases with secondary pneumonia, though this complication was seldom if ever mentioned by name. One of the most frequent causes of death was “chin cough & convulsion fitts.” In a letter from Boston dated September 23, 1782, Dr. Nathaniel W. Appleton said: “The chin-cough still continues—many have died in convulsions”;102 and in May, 1786, Dr. Holyoke said that “several of the younger patients were seized with convulsions, and a few carried off by them.”103
The incidence of the disease among adults was fairly high, though apparently not so high as with measles. Chalmers said that it “did not spare anyone who had not passed through it before,” and Holyoke added that several adults “suffered severely by it” during the 1786 epidemic in Salem. Inasmuch as there had been at least two previous epidemics in Salem (1770, 1782), one may conclude that most of these adults lived in isolated districts. But in spite of these references to adult cases, whooping cough must have been fairly common even in small towns, for most sources reveal that it was then, as now, predominantly a disease of childhood. Then also, as now, it was most fatal among infants. Out of one hundred deaths fifty occurred during the first year of life, and forty-one of these in the first six months.
Mumps
Mumps was known in this country at least as early as May, 1699, when John Marshall of Braintree entered in his diary: “I did not hear of any great matter which happened: only we had severall sick with an unusuall distemper called the mumps of which some weer bad. But none dyed, that I heard of.”104 Nicholas Gilman of Exeter was “exercised by the mumps” in June, 1726.105 According to Chalmers, there were epidemics of “Serous Quinsey” in South Carolina during 1744, 1768, “and at other times.”106 In 1777 there was an epidemic “of so-called Mumps, or badly swollen throat” among the Moravians of North Carolina:
[Salem, North Carolina] April 19 [1777]. Br. Preazel went to Bethania, and will hold the services there tomorrow, as since Monday Br. Ernst has not been able to leave his room on account of trouble with his feet. A certain disease is epidemic in that neighborhood, which they call Mumps; persons get a big swelling on the throat, and with others it affects the limbs.107
Two months later several brethren were still being “annoyed” in Salem, and at Nazareth Hall “not one of our Brethren, boys or children” escaped.108 According to Rush, there were epidemics of “cynanche parotidea” in Philadelphia during the winters of 1786–1787 and 1792–1793.109 The disease was also casually mentioned in the Holyoke (1763) and Patten (1776) diaries. One death from “mumps” was reported in Westborough in 1755110 and another in Philadelphia in 1782.111
Impaired only by the inclusion of swollen axillary and inguinal glands, Chalmers’s otherwise excellent account, wherein was mentioned involvement of the testicles and permanent immunity, was the only medical description of this disease published previous to 1800. Dr. Alexander King of Suffield had written an excellent account in his diary in 1784 but it was never printed.
Chicken Pox
Chicken pox is one of those diseases which were probably very well known to laymen long before medical men got around to writing them up in their books. Much has been made of the so-called “first” description by Dr. William Heberden of London in 1767, but good evidence that the disease was well known even in America long before Heberden’s time is contained in a charming, gossipy letter written by a twelve-year-old boy in East Windsor, Connecticut, on May 10, 1716. Informing his sister Mary, who was away at school, of all the newsworthy events of the neighborhood, he continued:
Abigail Hannah and Lucy have had the Chicken Pox and are recovered but jerusha has it now but is almost well I myself Sometimes am much Troubled with the tooth ack but these two or three Last Days I have not Been troubled with it but verry little so far as i know the whole famaly is well except Jerusha . . .
Your Loving Brother Jonathan E[dwards]112
The reason chicken pox was only occasionally and casually mentioned113 during the eighteenth century is that in comparison with other diseases it was very mild. Chalmers decided that it was “needless to say much” about it and gave it only a few lines. Naturally, because of the superfical similarity, it was occasionally confused with smallpox. Douglass said that during the “Small-Pox Time 1752, the Chicken or Spurious Pox was frequent, and sometimes passed for the Small-Pox, and some Persons have ineffectually been Inoculated from thence . . .”114 A more serious error was recorded by Mrs. Mary (Vial) Holyoke in her diary for January 25, 1764: “Mr. [John] Appleton moved to the pest house with the small pox which proved to be Chicken Pox.”115 Another instance in which the two diseases were confused was recorded in 1788;116 but since the average layman knew from bitter experience so much about the signs and symptoms of smallpox, indeed much more than the average doctor knows today, it is probable that this error did not occur very often. Only one instance of death from chicken pox has been found: a nine-months-old child died in Preston, Connecticut, on September 24, 1797.117
Dysentery
Bloody flux, once called the “most violent and dangerous of all American diseases,” should not be confused with the disease sometimes called “Common Flux” in Massachusetts or “Lax” in Pennsylvania, though in many records it is impossible to differentiate them. The latter disease, or nonspecific diarrhea, was seldom serious except among infants. Though occasionally mentioned in colonial records, it apparently did not receive much attention until described by Benjamin Rush in 1773. In the remaining years of the eighteenth century, as towns became more populous, summer diarrhea among infants was mentioned more frequently; but not until the nineteenth century, with its crowded cities, contaminated milk and water supplies, and poor sewage systems, did “cholera infantum” or “summer complaint” reach its peak. It is also important and equally difficult to differentiate bloody flux from typhoid fever because these two diseases had the same seasonal distribution, both produced gastro-intestinal symptoms, and both occurred in epidemic form. And here, too, one cannot find many good records of unquestionable typhoid fever until late in the eighteenth century unless one is willing to accept as typhoid fever some of those cases of “long fever,” “nervous fever,” or “bilious fever” that occur so frequently in the early records. Of the three diseases, bloody flux is the easiest to identify because of the following characteristics: fever, bloody stools, short duration when fatal, relatively high case fatality rate, deaths not limited to infants, occurrence during warm weather, and communicability as shown by multiple deaths in the immediate environment. In colonial records concerning flux at least three, preferably four, of these characteristics should be required for a diagnosis of bacillary dysentery, but at the same time it should be realized that if one’s postulates are too rigid, one will, because of inadequate details, overlook a good many widespread epidemics.
Dysentery is one disease that could have been easily imported because of its widespread distribution abroad and the unsanitary conditions aboard crowded ships. In fact, epidemics in this country can in many instances be directly traced to ships. In 1618 the Neptune and the Treasurer “brought a most pestilent disease (called the Bloody flux) which infected the whole colony [of Virginia]. That disease, notwithstanding all our former afflictions, was never known before amongst us.”118 Out of 180 passengers, “packed together like herrings” on the William and Thomas, bound for Jamestown in 1619, only 50 survived “the flux, and also the want of fresh water.”119 In October, 1699, an “over-thronged” ship, fourteen weeks out of Liverpool, arrived at Philadelphia having lost fifty-six passengers from “Fevers, Flux and Jaundice.”120 In August, 1732, Colonel Robert Carter of Virginia, after three days of sickness, “died of the Flux, which ’tis supposed he caught on board a Vessel from which he bought several Negroes.”121 In 1738 the St. Andrew, bound for Philadelphia, “lost 160 persons; another that arrived the day before lost over 150 . . . another has arrived, in which out of 300, only 50 fares are left. They have mostly died from dysentery, skin sickness and inflammatory fever; . . . Many of the survivors die after landing, and thus diseases are brought into the country, so that many inhabitants and landlords become sick, are seized by the epidemic and quickly carried off.”122 On a ship from Rotterdam that was obliged to put in at Block Island in 1739, out of four hundred passengers only ninety survived “the exceeding bad Feavor and Flux” that prevailed on board.123 Occasionally, unfavorable weather delayed some ships until the sick and starving passengers were reduced to eating rats. In Gottlieb Mittelberger’s journal there are detailed descriptions of the appallingly unsanitary state of the ships carrying German settlers to Philadelphia in the mid-eighteenth century.124
Since bloody flux was so easily imported, it is not surprising to find records of many epidemics throughout the seventeenth century. In Virginia, by the eighth of September, 1618, there was “sickenesse over the Land.” Three hundred settlers died in 1619. The population had increased to two thousand by 1621, but because of “contagious sicknesse; wch being encreased by the Infection brought in by some shipps, there dyed that year of mortallitie neare upon 600 more . . .”125 Descriptions of the Massachusetts Bay Colony epidemic in 1630 are also rather indefinite,126 but a probable diagnosis of bloody flux is based on its occurrence during the summer, high case fatality rate, multiple deaths, and “lameness”—a dysentery complication first described by Sydenham in 1672. In some early records, however, “lameness” meant nothing more than “weakness.”
“Fluxes and fevers [were] very dangerous” in Ipswich in 1640.127
Though John Hull’s brief note concerning an epidemic of “flux and vomiting” among the children of Boston during September and October, 1657,128 does not exclude so-called “summer complaint of infants,” excellent evidence of the widespread distribution of dysentery about that time is found in a letter from John Davenport to John Winthrop dated New Haven, August 4, 1658:
. . . in this sickly time when many are afflictively excercised, with grypings, vomitings, fluxes, agues and feavers, though more moderately in this Towne, by the mercy of God, then at Norwalke and Fairefield. Yong Mr. Allerton who lately came from the Dutch, saith, they are much more sorely visited there, then these parts are. It is said, that at Mashpeag [Newtown, Long Island] the inhabitants are generally so ill, that they are likely to lose theyre harvest, through want of ability to reape it.129
Davenport in 1660, Hull in 1661, and Megapolensis in 166130 refer to other epidemics of probable dysentery; and Hull and Danforth both mention the epidemic which occurred during the summer of 1669. Danforth wrote: “7m. It was a very sickly time, many being visited with gripings, vomiting & flux, with a fever, which proved mortal to many infants & little children, esp’ly at Boston & Charlstown, and to some grown persons.”131
Danforth mentioned another siege of “fluxes & vomiting at Boston” during September, 1671; and in 1672 Hull said that “Sundry persons died, in 7ber and 8ber, of voiding much blood and some worms,—persons of grown age and young men.” Josselyn, in his An Account of Two Voyages to New England (London, 1674), wrote that “griping of the belly (accompanied with Feavor and Ague) which turns to the bloody flux” was a common disease in New England and that it “together with the smallpox hath carried away abundance of their children.” Increase Mather, writing of the 1676 epidemic of “fever & fluxes (especially in Boston),” said that fifty persons died during August, eleven of them within two days; but at the same time, according to Samuel Hooker, the “bloudy flux” was not so mortal in Hartford.132
In one of his letters, Wait Winthrop mentioned still another epidemic in Boston during September, 1684; and it appears that “flux” caused many deaths during the so-called “bilious plague” in Philadelphia between August and October, 1699.133 A few months later a very unusual epidemic occurred in Bokton (Wilmington), Delaware:
There came upon us with the beginning of this year [1700] a severe and contagious sickness, dysentery, which especially in Bokton and round about was very violent and many of our congregation died, but none on this side the creek. Those who finally lived through, remained afterwards, overwhelmed with all sorts of difficulties in their bodies, with pains and lameness which kept them down mostly till about Easter.134
Of the scores of dysentery epidemics before 1800, this was one of the very few to begin during cold weather, and the explanation may be that it was a continuation of the epidemic that started in Philadelphia the previous autumn. Dysentery was so decidely a disease of warm weather that even in towns where it was widespread during two successive years it usually disappeared during the intervening winter and spring. It is also interesting to note that the writer said that the disease was contagious. Countless lives could have been prolonged had this idea prevailed and simple quarantine precautions been taken as during smallpox epidemics. Such measures would have been more effective because dysentery is more easily controlled. But no one ever suspected “healthy” carriers of dysentery, and the contagion theory thus never gained much ground. It was a full century later before it even became a subject for serious debate.
The century closed with another severe epidemic in Boston.135 In September, 1700, John Marshall wrote that “many persons dyed at Boston, especially children, of a bloody flux and feaver, and some dyed of it in the Country.” No doubt many other epidemics are hidden in the records, but from the evidence at hand one may conclude that bloody flux was one of the most formidable and widespread diseases of the seventeenth century.
Eighteenth-century dysentery epidemics were far too numerous for detailed accounts and, besides, in most diaries and newspapers one can find only a few sentences concerning even some of the most malignant ones. Seldom did anyone stop to describe the disease, for it was apparently assumed that everyone knew exactly what was meant by “bloody flux.” During the first third of the century there were many warm-weather epidemics accompanied by multiple deaths the causes of which, however, are still undetermined; but the diagnosis of dysentery is fairly well established for the rather severe outbreaks in Newark, 1704; Boston, 1711; South Carolina, 1715; New London, 1722; New York, 1731; and Virginia, 1732.136
A virulent dysentery swept through Boston in 1734. According to the Boston Weekly News-Letter, August 29, 1734:
After a Spring and Summer of extraordinary seasonable Weather, the like whereof scarce ever known, in these parts, as also a general measure of Health, it now, towards the close, begins to be very sickly, many both elder and younger Persons, being within a few Days taken down with a Fever and Flux, of which several have died after less than a Weeks Illness.
The sudden onset throughout the town makes it appear as though the infection had a common source. The most interesting item about this epidemic, however, is that an account of it, the first printed American account of the disease, appeared in the Boston Gazette of September 29, 1734. It was written by Dr. Thomas Harward, King’s Lecturer at King’s Chapel, and “Practitioner of Physic.” Apparently he contributed the same article to “Medical Memoirs,” the first number of a medical journal proposed by the first medical society in this country. Unfortunately, both items appear to have been lost.137
A serious epidemic in East Haven, Connecticut, began in August, 1742, and, like many other dysentery epidemics, returned the following summer, causing altogether forty-three deaths in a population of about five hundred.138 As illustrated in the graph, dysentery was sometimes more devastating than diphtheria. Here also are found the first good examples of dysentery multiple deaths: two children of Daniel Potter died on September 9; his wife and another child died on September 15; and a fourth child died on September 20. There were three deaths in both the Mallory and Moulthrop families, and two deaths each in the Austin, Roberts, Russell, and Smith families. A similar, though smaller, epidemic occurred at the same time (1742 and 1743) in East Hampton, Long Island.139
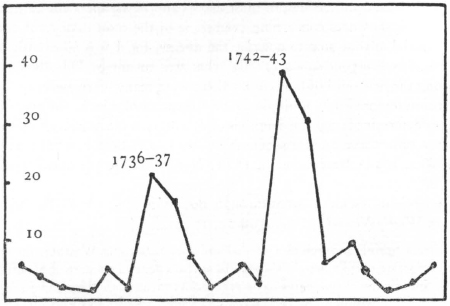
East Haven, Conn., deaths, 1730–1749
Diphtheria 1736–37; dysentery 1742–43
Cadwallader Colden said in 1745 that as long as he could remember, the northeast part of New York City had been subject to malignant dysenteries, especially among children.140 It was said that in 1745 “the town of Stamford in Connecticut was severely distressed by a malignant dysentery, which swept away seventy inhabitants out of a few hundreds. The disease was confined to one street.”141 In the same year dysentery epidemics started in Westborough, Massachusetts, and surrounding towns. The Reverend Ebenezer Parkman wrote in his diary:
September, 1745. 6th at Eve Mr Bezal Eager come from Mr Billings wth his Earnest request to have me go over to see his sick Children. I went and found his little son, his only son, very nigh to Death, and Two little Daughters sick—returned at abt ten & ½ to my Family. Their sickness is Fever & Flux wc greatly prevails in Shrewsbury and many Childr are taken away . . . 10th . . . my Wife and I went to the Funeral of Two of Mr Billing’s Children—his little son and a little Dauter who Sabbath was Sennight went hand in hand to ye House of G. now lay in one Grave & in one Coffin. They were buryed by the New Meeting House. The first yt have been buryed in that place . . . 12th Fast on the North side. Mr Cushing [of Shrewsbury] sent a Letter yt the Sick and Dead among ym prevented his coming. Mr Morse [of Boylston] sent a Letter also yt not only was ye most distressing Sickness among his nrs but he hims. was Sick nay and desired a Fast might be kept among them next Week . . . 16th Was at ye Funeral of anor of Mr Billings Children & Mrs Billings ill. N.B. A Story has got about of a Dream of Mrs Billings, & wc I took the Freedom to enquire into and wc she confirmed, viz yt she Saw a man bring ye Coffin of her youngest Child into ye House upon wc She looked on: but presently yre came in another Man wth a large Coffin, & said to her yt she had not need take on for her Child for here was a Coffin for her also, for she wd die next . . . N.B. Mr Hale who lives near ye new burying place (tis said) saw a large Coffin (as well as a small one) in ye air just over ye Burying place last Tuesday evg imedly after ye burying Mr Billings Two Childr. wc storys much fright pp abt Mrs Billings Death but I reply’d yt we have a more Sure word of prophecy &c. Mr John Oake & Mr Jesse Brigham have Each of ym a Child very bad of ye Distemper both wc I visited & prayd with. 17. I visited Eunice Bradish A.M. She lying Sick. Messengers one after anor of ye Deaths and Sickness among us. Mr Brighams & Oakes Childr dyd last night. Mrs Billings very bad. Mrs Dinah Goodenow taken last night, but better today.142
In near-by Sutton, on November 5, it was proposed to set aside a day of humiliation on account of “ye sickness.”143
The epidemic that began in Westborough about mid-August, 1746, was still worse than that of the year before. Parkman recorded that twenty-five children died within two months, among them four from the Barns family. Days of “Solemn Humiliation Fasting & Prayer on acct of ye great Mortality” were observed in Westborough (September 4), Hopkinton (September 18), and Northborough (September 22). Among the thirty-seven deaths in Harvard were five Willards, four Coles, four Sawyers, and three Warners.144 At the same time there were multiple deaths in many other Massachusetts towns, but the disease has not been identified though I suspect it was “Fever & Flux.”
Records of epidemics around 1750 are somewhat difficult to evaluate because both dysentery and throat distemper began appearing almost simultaneously in some towns. In his notes on the “bloody Flux” epidemic of 1747, Joshua Hempstead recorded at least three deaths from “Fever & Flux & Canker.”145 It is possible that thrush, a common complication of dysentery, may have been confused with “canker”; but inasmuch as throat distemper was common at that time, it seems fair to assume that the patients had both diseases. Noah Webster said that both dysentery and ulcerous sore throat were very fatal in Guilford during 1751, but a commemorative broadside146 states that the epidemic was caused by one disease; and the age distribution of the deaths (more adults than children) is very much in favor of dysentery. However, in Plainfield, Connecticut, while five members of the Dow family were dying from dysentery, three Woodwards in a house near-by were dying from “Canker” (1754).147 There are also a few family records showing multiple deaths in both spring and autumn of the same year, suggesting two separate epidemic diseases such as diphtheria followed by dysentery; but it is hazardous to guess the causes of either multiple deaths or epidemics without at least a few details. In spite of the confusion, epidemics definitely identified as dysentery occurred in Connecticut in Waterbury (1749), where 130 died, Woodbury (1749), where 57 died, Canaan (1751), where “a great many old people” died, Hartford (1751), where 64 died, and New Haven (1751), where 45 died.148 There were also severe epidemics in Fairfield during June and July, 1753 (which was a little off-season for a New England epidemic), in New London and Norwich during the mid-summer and autumn of 1753, and in Plainfield during 1754 and 1755.149 Concerning the Norwich epidemic Jabez Fitch, Jr., noted in his diary in 1753: “ye Later Part of this Sumer & ye Foll was ye Most Remarkable for Sickness that Ever was Known in this Plais In About 2 months 27 Persons Died of ye Camp Distemper In our Society.”150
After 1753 the name “camp distemper” became increasingly popular because of the prevalence of dysentery among troops. An epidemic of dysentery among Braddock’s forces undoubtedly contributed to his defeat.151 Very likely this was the disease to which George Washington referred when, on July 8, 1755, just after the disastrous battle of that campaign, he wrote to his mother: “. . . I was the only person then left to distribute the Genl’s. Orders which I was scarcely able to do, as I was not half recover’d from a violent illness, that confin’d me to my Bed, and a Waggon, for above 10 days; I am still in a weak and feeble cond’n . . .”152 The author of an article in Ames’s almanac for 1759 thought that more soldiers died from diseases in camps than fell on battlefields.
Not only did dysentery cause havoc among troops, but frequently when soldiers camped in or near a town, the disease quickly spread to the civilian population, particularly to children, who were less able to withstand it. Moreover, ailing soldiers were often sent home to recuperate, and thus the disease could have been carried to distant towns. Such was the case in one instance in Sutton, Massachusetts: “Oct. 21st [1758] This day sen’it died Mr. Hall, of the camp disease, lately returned from the army—sundry more are sick in the Town. Our forces are coming from the lake without further attempts on Ticonderogue.”153
The year 1756 was a perilous one for the children of Massachusetts. It would not be surprising to find that well over a thousand of them died in this one colony alone. The throat distemper was not so bad as usual, but it was bad enough. Most of the trouble started, however, after the middle of July, when multiple deaths began to increase in number. In Newton five Sheppard children, in Oxford four Parker children, and in Weston four Smith children died during August and September. During October and November four Lealands died in Sherborn, four Robinsons in Dudley, and four Johnsons in Southborough. At least one hundred families lost two or three. The cause has not been determined in all cases, but a detailed account of the epidemics in some small towns north of Worcester has been preserved in a sermon by the Reverend John Mellen of Lancaster.154 He started off in the usual tough Calvinistic fashion but managed to include some interesting footnotes:
I write unto you little Children, because I wou’d move you to Consideration and Seriousness, to reflect upon yourselves, upon your Ways, upon the End of Things, upon Death, Judgment and the eternal World, and to prepare for your own Death and Dissolution. I write unto you because I am tenderly concerned for you, and pained at my Heart for that dreadful Destruction that God has made among you, within a few Weeks past, by an obstinate and noisome Disease, that has bid such Defiance to Medicine . . .
How we have attended Funeral upon Funeral, Day after Day, and Week after Week; and laid our Hopes in the Grave . . . How sudden the Deaths! How awfully distressing the Sickness of the Deceased! . . .
And how that in the Autumn . . . [of] Seventeen Hundred fifty-six, the Inhabitants of the Land, and more especially those in the Neighbourhood of this Chasm, were seiz’d with this mortal pestiferous Distemper, that has swept them off in such Numbers.
The Distemper is a Dysentery, or Bloody-Flux. And when malignant, is commonly attended with Vomiting, high Fever, extream Pain: and sometimes with visible Canker.—When the Patient appeared with high Symptoms of the Distemper at first, he often died in 3 or 4 Days: Others, and especially those less violently seiz’d, lived 8 or 10 Days, or more. Much vomiting a bad Symptom: and cold Hands and great Restlessness commonly fatal: Tho’ many died without all, if not without any, of these Symptoms in a high Degree . . .
In this Parish have been buried 42 in about seven Weeks [thirty-three of them children]. A Mortality, (which in less than three Years wou’d have buried the whole Parish, which consisted of near 800 Souls), allowing for the probable Increase in the mean Time. The Proportion of the Dead to the Living is as 1 to 19, nearly. In the little Town of Holden [population about four hundred], where the Sickness first began, which, [to] the 20th of October had buried 40, the Proportion is much greater. In Old Rutland [population about nine hundred], at the same Time, had died 45. In the North Parish in Shrewsbury upwards of 20. And in more distant Places less, in Proportion to the Number of People.155
This same epidemic spread to Westborough. Ebenezer Parkman, recording the names of those who were sick or dead, turned back a few pages of his diary to September 13, 1756, to make a marginal note: “The Beging of ye sore sickness.” Of some significance, perhaps, was his remark that Dr. Gott had returned to Marlborough “from ye camp” and that “The sorrowf. news from ye Army is confirmed, of ye multitudes wc have dyd by Sickness.” Early in October he noted that eight persons died within four days. There was a fast in Shrewsbury on October 13, and another the following day in Westborough. In Chauxit (now Sterling) five percent of the population died within eight weeks, “and the well hardly sufficed to give proper care to the sick.” In Harvard there were about twenty-five more dysentery deaths during September and October.156 Other Massachusetts towns suffered epidemics during the autumn of 1756; and in Maine “the slow fever and bloody flux” prevailed at Black Point, North Yarmouth, and Falmouth.157
Then followed a relatively calm period so far as dysentery is concerned. There were occasional single and multiple deaths and even a few small epidemics in New England; but with the exception of a terrible epidemic in New York158 late in the summer of 1767, when fifteen deaths were reported daily, there was nothing of great interest until 1769.
During August and September, 1769, the real, devastating bloody flux broke out again in Guilford, Connecticut, and in Pennsylvania.159 At the same time large numbers of children died in Boston, Marblehead, and Salem;160 but from the information now available it is impossible to exclude so-called “summer complaints of infants.” This is particularly true of Boston records because after similar increases in deaths had occurred during the late summers of 1772 and 1773, the newspapers began to speak of “The Disorder that generally attends young Children at this Season.”161 There is less doubt, however, about the diagnosis in other towns, particularly in Danvers where there was “Extraordinary Sickness and Mortality [from] Bloody flux & fevers” during 1773. Both smallpox and dysentery contributed to the increase in deaths in Salem, and, according to Dr. Holyoke, the dysentery was very fatal. Noah Webster said that in New Haven and East Haven the dysentery was also of a “peculiarly malignant type.”162 During 1774 “hemorrhoidal diarrhea” was common in North Carolina; and in Rehoboth, Massachusetts, during October, “Fever & Flux” claimed five children belonging to Daniel Bliss.163
If ever there was a dysentery year in New England, it was the memorable year of 1775. On the surface it seems that during this and the next three years dysentery caused the deaths of more children than all other diseases combined. At this late date, chiefly because the newspapers of that time were devoted almost exclusively to war and politics, it is difficult to find detailed descriptions of many local epidemics; but it was a rare New England town that sometime during these four years did not experience an epidemic that would begin in mid-summer, reach its peak in autumn, and disappear in winter, meanwhile killing off children in groups of twos and threes and fours. Occasionally, in some towns, the epidemic would last two summers, while in other towns there would be two separate epidemics, one in 1775 and another in 1778. Altogether it was one of the most fatal periods for children in colonial history.
As early as June 17, 1775, the “Bloody Flux [was] already very bad in Maryland.” Early in August, Philip Fithian made another note in his diary: “. . . many Disorders, chiefly the Flux, are now raging in the lower Counties, Chester, Newcastle &c. I pray God Delaware may be a Bar & stop that painful & deadly disorder. Enough has it ravaged our poor Cohansians . . .”164
It was characteristic of dysentery years for the disease to break out in the southern and middle colonies before it broke out in New England. But also contributing greatly to the magnitude of the New England epidemic were the British troops in Boston and the American troops in Cambridge. The first reports of the disease appeared in the newspapers during July: “We hear the camp distemper rages in the regular army in Boston, as also among the distressed inhabitants who are confined in that town by order of Tom. Gage, in open violation of his most solemn engagement. It is to be hoped he will meet the fate of Pharoah of old, whose example he so exactly follows.”165 In August a letter sent through the lines mentioned that two members of the Cotton family and two of the Wiswall family were dead of the flux.166 It was also learned that three thousand British troops were sick.167 Apparently by the end of August the disease had appeared in many inland towns, for there was published on the front page of the Massachusetts Spy a whole column of medical news entitled “A Cure for the Bloody Flux.”168
Benjamin Rush was responsible for the statement that there was scarcely any sickness in the American Army while it was in Cambridge; but other writers, including Dr. John Morgan, who was at the scene, said that army hospitals were crowded and that contagious diseases, including dysentery, were rampant.169 Certainly if this army camp was anything like the others during 1776 and 1777, conditions were deplorable. It has been authoritatively stated that more wounded men died from contagious diseases after they reached army hospitals than died from the effects of their wounds. Noah Webster, who did not believe that dysentery was contagious and who ridiculed all his contemporaries who disagreed, tried to prove that the Army was not responsible for the spread of dysentery to civilians by pointing out that there were malignant epidemics during 1773 and that even some 1775 epidemics could have had no relation to returning soldiers. But Webster had no conception of “healthy” carriers, and carriers were undoubtedly a major source of trouble. It is difficult to prove this by the evidence now at hand, but there are a few suggestive items. It so happens, for instance, that the first deaths in the Marlborough epidemic of 1775 were in the family of Colonel Abraham Williams, and there are other instances of multiple deaths of children whose brothers or fathers were serving in the war, such as those of four members of Captain Arthur Daggett’s family in Sutton. There are also a few records of soldiers taken sick in camp and returning home to die. In Newbury, John Pearson died on September 28, 1775, “of ye dysentery, being bro’t home sick from ye army at Cambridge.”170 Nathan Stone, thirty years old, died in August, 1775, from “Camp Disease” while on his way to his home in Sutton, but he “got no further than Weston.”171 Dr. Matthew Irvine, a physician in Benedict Arnold’s ill-fated campaign into Canada—it failed, by the way, mostly because of dysentery and other contagious diseases—was stricken with dysentery “on the march from Cambridge.” Amos Farnsworth of Groton went home from Cambridge suffering from “Camp Fever.”172 It makes little difference whether or not the Army got its dysentery from British or American sources, for the fact remains that the Army, once infected, was the source of many disastrous local epidemics. The best evidence of this is from the autobiography of the Reverend Samuel West, minister at Needham in 1775:
The Dysentery soon prevailed in the American Army & extended itself more or less through the Country. Although it prevailed most in the Town near camp, my Parish partook largely of this calamity. We buried about 50 persons in the course of the season. Some families were dreadfully bereaved. One in particular a Mr. Joseph Daniels buried an amiable wife & 6 very promising Children in about 6 weeks—we often buried 3 or 4 in a day. My time was wholly devoted to visiting the sick, attendance on the dying & the dead.173
Writing to her husband about the sickness in her family, Abigail, wife of John Adams,174 vividly described the epidemic in Braintree. “The desolation of war is not so distressing as the havoc made by the pestilence. Some poor parents are mourning the loss of three, four, and five children; and some families are wholly stripped of every member . . . ’Tis a dreadful time with the whole province. Sickness and death are in almost every family. I have no more shocking and terrible idea of any distemper, except the plague, than this.”
The Marlborough records are complete enough to show that the epidemic in that town was the “most destructive” in its history.175 Out of a population of one thousand four hundred there were seventy-eight deaths during 1775, perhaps fifty from camp distemper.
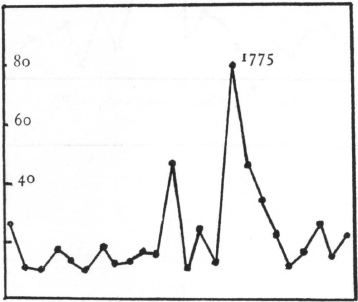
Marlborough, deaths, 1760–1783
The vital records show many multiple deaths.
In Dedham, on August 29, 1775, there was a “Parish Fast on acct of the mortal Dysentery” which had been raging for at least a week;176 and in Groton, Medford, and Sutton the epidemics appear to have been severe.177 Those in Brookline, East Bridgewater, Tewksbury, and Wakefield appear less serious on the basis of incomplete records. Of the more than twenty-five still unidentified but simultaneous epidemics, the worst were in Bellingham, Brimfield, Chelmsford, Medway, Plympton, Sharon, and Westford.178 In addition there were scattered dysentery deaths but no evidence of serious epidemics in numerous other towns in eastern Massachusetts. A Thanksgiving proclamation dated November 4, 1775, mentions the “wasting sickness . . . in many of our Towns,” although by that time it was apparently subsiding, for the “voice of health” was once again being heard.179
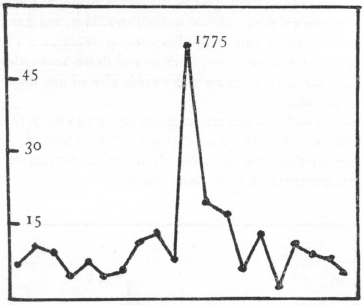
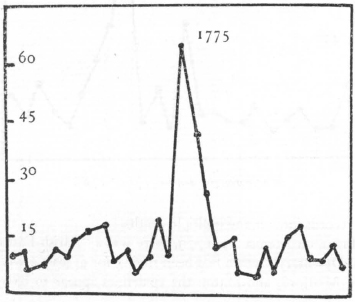
Coventry, Conn., deaths, 1760–1789
In Connecticut, according to Noah Webster, there were one hundred dysentery deaths in Danbury;180 and in Middletown dysentery followed in the wake of “cynanche maligna” in the spring.181 There were severe epidemics also in Wethersfield, Wintonbury, and, particularly, Coventry.182 The Reverend Solomon Williams preached a sermon on December 3, 1775, on the abatement of the “sore sickness” accompanied by multiple deaths in Lebanon and “in many towns.”183
If there is any question about dysentery in the Army during 1775, at least there can be no doubt about it during 1776. In June, Captain John Lacey wrote in his journal that the New England camp on Long Island was full of “Fluxes, Fevers, & Smallpox.” In July “The General [was] pained to observe” the frightful condition of the latrines and ordered all filth in and about the camp to be buried daily. The Chief Surgeon of the Hessian forces said that after they arrived in July, hardly a man escaped without dysentery or fever. Young Philip Fithian, describing the American military hospitals in New York, said: “In every apartment are many with the Dysentery”—and this was just before he himself contracted the disease and died. Dr. Ebenezer Beardsley also said that dysentery was rife in the Army during July, August, and September.184 James Tilton described the condition of the camp at King’s Bridge: “All manner of excrementitious matter was scattered indiscriminately throughout the camp . . . A putrid diarrhea was the consequence. The camp disease, as it was called, became proverbial. Many died, melting as it were, and running off at the bowels.” On October 4 Washington’s order of the day called attention to the “shameful inattention in some camps, to decency and cleanliness.” At that time it was estimated that one-third of his forces were unfit for duty because of sickness.
Elsewhere, too, there was ample reason to fear “more loss of men from Camp sickness than from ye Gun & Bayonet.”185 The Reverend Ammi Robbins, heartily distressed “midst sickness and death” while with the forces around Lake George, described the men, first terror-stricken by smallpox in April, then decimated by camp distemper throughout the summer.186 At one time less than 50 out of a force of 240 men were able to carry on. At the peak of the epidemic five men were being buried daily. Webster was an eyewitness to the “terrible fatal” dysentery among the troops at Ticonderoga. “I was at Mount Independence in October, and witness to the ravages of the disease. Of thirteen thousand troops, it was said that one half were unfit for duty.”
“The dysentery which prevailed in most parts of the United States in the year 1776” was said to have been “very mortal” in Kingston, Massachusetts, but neither in Kingston nor in other Massachusetts towns do my records reveal any terrible epidemics unless the one in Chester, in western Massachusetts, was caused by that disease.187 In West Hartford, Connecticut, a two-year epidemic started with the deaths of about twenty soldiers “in ye Camp,” but most of the multiple deaths among children occurred the following summer.188 There was another moderately severe epidemic in Middletown. In one parish in Morristown, New Jersey, there were twenty-five dysentery deaths including those of five members of the Reeve family and four Pruddens.189 All in all, however, there was nothing comparable to 1775.
The American soldiers at Lake Champlain suffered severely from dysentery during 1777. Burgoyne also had plenty of sickness among his troops. Baroness Riedesel, who was with the British forces, described what she saw on the night before the crucial battle of that campaign: “The whole entry was filled with the sick, who were suffering with the camp sickness, a kind of dysentery.”
In the new settlements of Vermont dysentery raged with “great severity” during 1777.190 In Athol and surrounding towns in Massachusetts there were numerous deaths from some epidemic disease, with a clue to the diagnosis furnished by the Royalston records, which show at least forty deaths from dysentery in a population of about six hundred.191 In Granville, too, the camp distemper was very bad.192 Similar but smaller epidemics occurred in some small towns in the Berkshires. In western Connecticut, particularly in Norfolk, Litchfield, and Fairfield, there were some dreadful epidemics.193 That in Norfolk was said to have destroyed ten percent of the population.
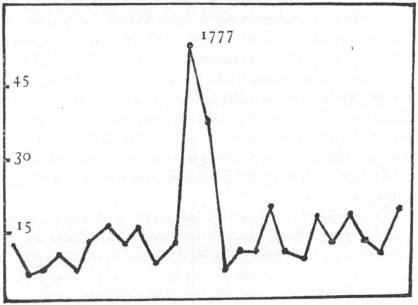
Norfolk, Conn., deaths, 1766–1790
The summer and autumn of 1778 was another trying period for the children of eastern Massachusetts. Smallpox and “slow fever” (typhoid?) were rife, but the East Bridgewater, Ipswich, Lynn, Medford, Spencer, and Tewksbury records show definitely that dysentery had again reached the epidemic stage. Not yet identified beyond doubt, but having all the characteristics of dysentery, were the fairly severe epidemics in Chelmsford, Dunstable, Harvard, and Lexington,194 and the less severe ones in Carlisle, Sherborn, and Woburn. Multiple deaths between August and November can be found in the vital records of at least twenty other towns. During this period six members of the Childs family in Lexington and five of the Fletcher family in Chelmsford died. The Larkins of Lancaster, the Merrills of Methuen, and the Newtons of Milford lost four apiece. In Plainfield, Connecticut, one branch of the Mordock family was destroyed. The story can be briefly summarized by a few words from the diary of the Reverend Thomas Smith of Falmouth, who wrote on September 30, 1778: “There is a terrible dysentery that prevails and rages at the westward. There is not a child three years old left in Mystic.”
The period from 1779 to 1793 throughout most of the United States, particularly New England, appears to have been relatively free from destructive, widespread epidemics. That is not to say that the disease had disappeared, for it was still present among the troops in the Carolinas during 1780 and in Virginia during 1781; and even considering the possibility of faulty diagnoses, one can still find occasional dysentery deaths here and there every single year. There are also numerous suspicious multiple deaths in various vital records, and there are even some indications that the disease may have been endemic in some of the larger towns. In the only available Salem records, for instance, there were six dysentery deaths in both 1782 and 1783;195 and Benjamin Franklin said in 1784 that dysentery was among the most common diseases of Boston.196 But during all these fourteen years less than a dozen serious epidemics have so far come to light, and though a few of them were frightful, they were all fairly well localized and scattered. Among the worst were those in Pennsylvania (1779), Sterling, Massachusetts (1786), Norfolk, Virginia (1787), Bennington County, Vermont (1788), Boston (1789), and Philadelphia (1791).197 Though the disease may have been on the wane, it was still regarded with utmost respect, for every now and then there appeared in the newspapers some sure-fire cures for the fatal “bloody flux.”
In the closing years of the eighteenth century, however, there were some of the worst epidemics of all; at least, they were so described. In Georgetown, D. C, and vicinity during 1793, the epidemic “swept away many hundreds.” In Caroline County, Maryland, there was “considerable mortality”; and in several villages of Pennsylvania there was “a malignity and mortality, unknown before in any part of the state.” It was also a “very sickly” time in Plymouth, Massachusetts. The disease was “more obstinate” than usual in Newport, Rhode Island; and in Coventry, Connecticut, it “killed almost every person whom it seized.”198
The year 1794 was not too dreadful, most of the known epidemics being limited to New Haven and Fairfield counties, Connecticut.199 Morristown had a small epidemic, its first since 1777. During 1795 Sterling, Massachusetts, New Haven, East Haven, and Branford, Connecticut, Dutchess County, New York, and Baltimore were the hardest hit.200 The disease was “never so alarming” as it was during 1796 in Castleton and Stockbridge, Vermont, and towns near-by. Forty-four persons died in Sheffield, Massachusetts, where the mortality was “perhaps unequalled in the annals of our country.” Fifty-nine died in Worcester.201 During 1797 Hanover, New Hampshire, had its first attack, and many Rhode Island towns were stricken.202 It was said that during 1798 the disease “spread over the country,” but I have records of only a few New England epidemics.
This is by no means a complete account of eighteenth-century dysentery epidemics, for not many towns remained free from an invasion of this dreadful “wasting disease.” Some towns suffered repeated epidemics, sometimes in successive years and again the following decade. During an epidemic of average severity half, or nearly half, of all the inhabitants of a town would become infected, and of these, one out of every six or seven would die. The net result would be a loss of five to ten percent of the population, to say nothing of the hundreds who barely escaped with their lives. Nor do these figures take into account the many thousands who must have died during nonepidemic years, particularly when so large a proportion of the population must have been innocent carriers. This was the disease that year after year made August and September the most dangerous months in New England. It was a disease of the aged, of young mothers, as well as a disease of childhood. One need only read some detailed first-hand accounts of the fear, sadness, misery and multiple deaths that always accompanied these frightful epidemics to realize that, while not like smallpox, a spectacular disease that generally made the headlines, dysentery nevertheless surpassed all other diseases as a cause of childhood deaths.
Smallpox, influenza, and tuberculosis should certainly be included in the list of common diseases of colonial children. A surprisingly large proportion of them also had worms. Death frequently followed from eating poisonous berries, thornapple seeds, and so-called “mushrooms.” Hardly a year went by without a report of a child fatally burned from playing with candles or gunpowder or from falling into open fires. More were drowned from falling off wharves or into unguarded wells or from swimming in treacherous streams. Still more were seriously, if not fatally, scalded from falling into large caldrons of boiling milk or water. And finally, when one considers that in addition to all these hazards, an incalculable number suffered from other serious noncontagious diseases and particularly “convulsion fitts,” it seems a little surprising sometimes that any of them survived.