 J. WORTH ESTES
J. WORTH ESTES  *
*
Therapeutic Practice in Colonial New England
MOST of what we know about the practice of medicine in eighteenth-century America has come from what colonial doctors said they did or what they recommended that others do. We have made most of our inferences about colonial therapeutics from physicians’ letters and books, both those they read and those they wrote.
However, it has not been documented that colonial physicians were uniform in their practices, that they actually did what they said they did, or that they carried out the recommendations of even the most authoritative writers. In addition, the colonial practitioner could be expected to use drug plants that were indigenous to the New World but unknown in the Old.
This study was designed to test the hypothesis that we can reconstruct the collective routine, everyday practice of colonial physicians from their account books, ledgers, and day books. Ideally, of course, we can best understand why a colonial physician prescribed the drugs he did only when we know the diagnoses, or the physical findings, he made before prescribing treatment. Unfortunately, such data are rare.1 Dr. Edward Augustus Holyoke of colonial Salem kept books from which this kind of information can be extracted, but the magnitude of the effort needed to do so outweighs its potential benefits because of the complexity of Holyoke’s records.
The greater part of the surviving useful data may be found in the account books in which physicians tabulated the treatments given each patient so that an appropriate person could be charged for the service rendered. From some of these accounts it has been possible to determine what they can tell us about therapeutic procedures common in colonial New England.
materials and methods
Colonial medical account books can be found in many local and regional collections, such as the Essex Institute, the American Antiquarian Society, and Old Sturbridge Village, as well as in medical collections, like those at the Boston Medical Library. The account books of Dr. Josiah Bartlett of Kingston, New Hampshire, cover perhaps the longest time span. They have been made available recently in the microfilm edition of Bartlett’s papers published by the New Hampshire Historical Society and the New Hampshire Bicentennial Commission, in which his accounts occupy 1237 microfilm frames, each of which reproduces two manuscript pages. Because of the extraordinary span of Bartlett’s accounts, which cover thirty-seven years with no hiatuses other than those necessitated by his visits to Philadelphia and elsewhere on official business, they were taken as the standard with which other account books could be compared.
Three eighteenth-century ledgers in the Boston Medical Library were selected for comparison with Bartlett’s. The ledger of Benjamin Rowe, Jr., of East Kensington, New Hampshire, for seven years, represents a second rural New Hampshire practice. And, in order to explore contemporaneous medical practice in Boston, the largest town in New England, the ledgers of Drs. William Aspinwall and David Townsend were chosen for study.
The two New Hampshire ledgers are accounts of day-by-day transactions. The two Boston ledgers, by contrast, contain entries for one or more families on each page, to facilitate billing heads of households at appropriate intervals. Because the account books were organized differently, the information available from each differed slightly. When possible, the following data were tallied from all four ledgers for each patient seen: sex, age group (child or adult), office call or house call (“visit”), name(s) of drug(s) administered, number of drugs administered, operations and other “surgical” treatments (e.g., bleeding, tooth extraction, dressing, reduction of fracture or dislocations), and professional fee. No data pertaining to clinical diagnoses were included regularly in any of the ledgers. The organization of the two Boston ledgers precluded analyses of the daily work loads of the two physicians or of the number of drugs that one of them (Aspinwall) prescribed for each patient. A ten percent sampling (every tenth microfilm frame or double page) was made of three ledger sets; thirty percent of Townsend’s ledger was sampled, because his handwriting was larger than those of the other three physicians, so that he made fewer entries on each page.
Because Bartlett’s ledgers covered such a long period, and in order to ascertain whether he employed any of his therapeutic agents with increasing or decreasing frequency over those thirty-seven years, the data from his ledgers were segregated by consecutive quarters of his ledger pages. As Table I shows, the number of patients represented decreased in each successive fourth of Bartlett’s ledgers. The modest decrease in the middle two quarters is largely attributable to the increasing number of nonprofessional transactions, including entries for payments of old debts, often in kind or services, on each ledger page. The substantial decrease in the last quarter of the ledger pages studied was caused by the doctor’s assumption of several political roles that required his absence from Kingston.
The drugs listed by each of the four physicians were “decoded” with James Thacher’s American New Dispensatory of 1810.2 This compendium can be taken to represent what had been common therapeutic practice for the previous half century. It provides information about the ingredients and clinical uses of about ninety-five percent of all drugs listed in the four physicians’ ledgers. Almost all the rest could be decoded with other standard reference works. The pivotal role of Thacher’s Dispensatory for this study is based on the assumption that it accurately reflects late colonial therapeutics. Because Thacher was a New Englander, a military surgeon, a biographer, and an active member of his state’s medical society, it seems reasonable to use his book as a standard guide to the vocabulary of colonial New England therapeutics. A glossary of the drugs listed in the four ledgers is included as Appendix I to this paper.
Because it was not possible to relate drug usage to clinical diagnoses, Thacher’s outline of drug classes was employed in order to provide a uniform guide to the probable pharmacological (but not clinical) indications for the use of each drug by the New Hampshire and Boston physicians. The drugs they prescribed or dispensed were segregated according to the first class to which they were assigned by Thacher. (He assigns some drugs to more than one class. Although these are noted in the tabulation of the drugs used by the four physicians, further analyses by other secondary drug properties were not made.) In spite of the potentially tenuous assumption involved in this manner of analyzing the physicians’ practices—that each doctor used any given drug for only the same indication—the uniform application of Thacher’s primary drug class attributions should mitigate the magnitude of erroneous inferences made from the data. At any rate, in the absence of other external standards, or of clinical diagnoses for each patient, Thacher’s compendium provides the only available baseline for assessing the uses to which drugs were put in colonial New England.
Another kind of clue for testing the homogeneity of medical concepts and experience in the late eighteenth century is provided by the bills of mortality for the communities in which the subjects of this study practiced. Bills of mortality for Kingston, Dover, and Hampton, New Hampshire, provide information about Josiah Bartlett’s patient population, which included patients from all three towns. The bill of mortality for Kensington, New Hampshire, reflects the medical milieu of Benjamin Rowe of East Kensington. Bills for Boston, and for Portsmouth, included to represent New Hampshire’s largest town, one in constant communication with Boston as well as with the rest of New Hampshire, date only from the first two decades of the nineteenth century. However, there is no a priori reason why these early nineteenth-century bills cannot be taken to represent medical thought in those same communities for the proceding half-century, the period of the four sets of ledgers studied.
Most of the statistical analyses used involve conventional methods for calculating regression and correlation coefficients.3
biographical data
Josiah Bartlett (1729–1795) was born in Amesbury, Massachusetts, where he was tutored in medicine by Dr. Nehemiah Ordway, a distant relative. Bartlett opened his practice in Kingston, New Hampshire, in 1750, where he remained until he died. Never a regular military surgeon, in either the French and Indian or Revolutionary wars, he was very active in his state’s politics. He was, in turn, a selectman, justice, delegate to the colony’s Provincial Congresses and to the Continental Congress, signer of the Declaration of Independence, and first governor of New Hampshire. Bartlett was also a charter member and first president of the New Hampshire Medical Society (1791).4
Benjamin Rowe, Jr. (1750–1818), was born in Kensington, New Hampshire, where he studied medicine with his father. The son practiced in East Kensington from 1771 until his death, although he was a surgeon’s mate during the Revolution.5
William Aspinwall (1743–1823) of Brookline, near Boston, graduated from Harvard College in 1764. He studied medicine with Dr. Benjamin Gale in Killingworth, Connecticut, and with Dr. William Shippen, Jr. at the Pennsylvania Hospital in 1769. A surgeon to the patriot troops at the siege of Boston, Aspinwall was an active inoculator and, later, vaccinator, for smallpox. He was also active in state and local politics, while maintaining a busy practice in Brookline and Boston. He was elected a fellow of the Massachusetts Medical Society in 1812, and was awarded an honorary M.D. from Harvard in 1808.6
David Townsend (1753–1829) was born in Boston, where he studied with Joseph Warren after graduating from Harvard College in 1770. Townsend became a senior medical officer during the Revolution, and was later physician-in-chief of the U.S. Marine Hospital at Chelsea, near Boston. His patients included many of the town’s most prominent citizens, such as Governor John Hancock. Townsend joined the Massachusetts Medical Society in 1785. The only one of the four physicians included in this study to publish a book, his was a nonmedical religious tract called Gospel News.7
results
Demographic Properties of the Four Practices
Of the 7095 patient visits included in the samples from the four physicians’ ledgers, fifty-two percent were Bartlett’s, sixteen percent were Rowe’s, twenty-one percent were Aspinwall’s, and eleven percent were Townsend’s. As Table I shows, adult men constituted the majority among the three practices for which data pertaining to age and sex are available. Children were less numerous in Dr. Rowe’s practice than in Dr. Bartlett’s, both in small New Hampshire towns. Over the thirty-seven years of Bartlett’s ledgers, the proportions of women and children increased; perhaps they were artificially low during the first years of his career, before his skills became recognized and accepted. Because both he and Rowe were the only physicians in their respective communities, we wonder who took care of the children in East Kensington or whether, in fact, their parents even sought professional medical help when the children were ill.8 Perhaps another physician in Rowe’s area “specialized” in the care of sick children, an inference suggested by the fact that Rowe saw only about two-thirds as many patients each day as did Bartlett. It is most likely that Rowe’s patients were drawn from a smaller population than Bartlett’s, whose patients came not only from Kingston but also from surrounding towns, like Dover, Hampton, and Newmarket. Unfortunately, it is not possible to estimate the number of patients seen daily by the two Boston physicians.
Demographic properties of the practices of four colonial New England physicians, collated from data in their ledgers.
| Josiah Bartlett | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Quarter of ledger pages tallied | ||||||||||
|
I |
II | III | IV | Total |
Benjamin Rowe, Jr. |
William Aspinwall |
David Townsend |
|||
|
Jun. 1751–Jul. 1758 |
Sep. 1758–Apr. 1764 |
Jun. 1764–May 1770 |
Aug. 1770–Dec. 1787 |
Jun. 1751–Dec. 1787 |
Jun. 1785–Jul. 1791 |
1782–1795 |
1784–1791 |
|||
|
Period of ledger (s) |
||||||||||
|
Total number of patients seen |
1196 |
984 |
928 |
593 |
3701 |
1161 |
1454 |
779 |
||
|
% Patients* who were: |
Men |
71.8% |
48.5% |
46.9% |
50.0% |
55.9% |
87.1% |
— |
66.4% |
|
|
Women |
15.0% |
26.8% |
27.9% |
32.0% |
24.2% |
12.6% |
— |
20.5% |
||
|
Children |
13–2% |
24.7% |
25.2% |
18.0% |
20.0% |
0.3% |
— |
13.1% |
||
|
Mean number of |
||||||||||
|
patients seen |
5.1 |
4.9 |
5.7 |
1.7 |
4.4 |
2.9 |
— |
— |
||
|
per day (± s.d.) |
±2.5 |
+2.2 |
+4.2 |
±1.4 |
±2.3 |
±0.9 |
— |
— |
||
|
Mean number of |
||||||||||
|
house calls per |
2.1 |
2.0 |
2.1 |
0.7 |
1.7 |
1.7 |
— |
— |
||
|
day (± s.d.)† |
±1.4 |
±1–3 |
±1.8 |
+0.7 |
+1.3 |
±0.7 |
— |
— |
||
Sources: See text.
* Among patients whose age and sex can be ascertained from the ledger entries.
† All four physicians often saw more than one patient during each house call.
As Table II shows, the populations of both Kingston and Kensing ton were relatively stable during Bartlett’s and Rowe’s lifetimes. After the turn of the century, Kingston’s population even fell by a modest amount. By contrast, Boston’s population was increasing rapidly. Although the town’s prewar population had fallen by about two-thirds at the end of the siege of 1775–1776, by the time of the Aspinwall and Townsend ledgers it was increasing rapidly, by about a third over the last decade of the eighteenth century.
Populations of Kingston, Kensington, and Boston in the late eighteenth century.
| Kingston | Kensington | Boston | |||
|---|---|---|---|---|---|
| Date | Population | Date | Population | Date | Population |
|
1757 |
ca. 950 |
1775 |
797 |
1755–64 |
15,631 |
|
1773 |
989 |
1790 |
800 |
1765–74 |
15,520 |
|
1775 |
961 |
1790 |
18,038 |
||
|
1790 |
906 |
1800 |
24,937 |
||
|
1810 |
746 |
||||
Sources: Jeremy Belknap, The History of New-Hampshire, 2nd ed., 3 v. (Boston, 1813), iii, 228; Timothy Dwight, Travels in New England and New York, 4 v. (1821–22; rev. rpt. ed., Cambridge, Mass., 1969), I, 301; Frank C. Mevers, ed., Microfilm Edition of the Papers of Josiah Bartlett (1729–1795) (Concord, N.H., 1976), frame 3075, and Guide, 11; Lemuel Shattuck, The Vital Statistics of Boston (Philadelphia, 1841), xii–xvii
Bartlett has provided us with one tabulation of the population of his own town, one that he made in his capacity as a Kingston selectman in 1773:
|
Unmarried men 16–60 |
110 |
|
Married men 16–60 |
142 |
|
Boys 16 Years & under |
201 |
|
Men 60 Years & upwards |
41 |
|
Females Unmarried |
295 |
|
Females Married |
172 |
|
Widows |
23 |
|
Male Slaves |
3 |
|
Female Slaves |
2 |
|
TOTAL |
969 [sic] |
Although Bartlett’s arithmetic failed him (the actual total is 989), the age and sex distribution of Kingston’s population was like that of all New Hampshire. The town’s doctor served a population of about 1,000, plus his patients who lived in neighboring communities. This physician-to-population ratio is like that found in Portsmouth (whose population was 5,000) at the same time, and probably in eighteenth-century America as a whole.9 Boston’s population was about twenty times larger than Kingston’s, and boasted an even greater ratio of physicians to population, as Eric H. Christianson has shown elsewhere in this volume.
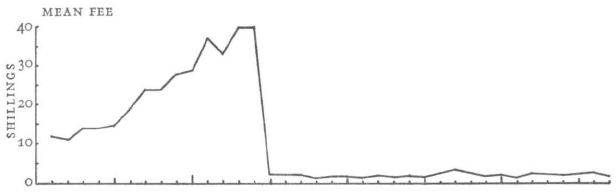
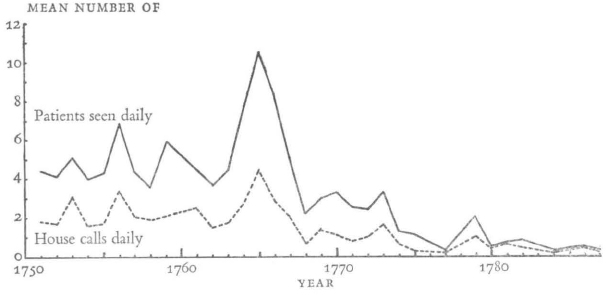
Graph 2 shows fluctuations in the average number of patients that Bartlett saw each day. His practice increased most during epidemics, reaching its peak work load just after the French and Indian War, when both poverty and disease were widespread.10 Bartlett’s growing involvement with public service and then in revolutionary politics eventually curtailed his opportunities to see patients, although he did see some throughout the entire period of his ledgers. During the last years of his practice, Bartlett was seeing fewer patients than Rowe was at the same time (Table I), but both men were making similar numbers of house calls each day. It was not possible to determine the daily number of house calls in the two Boston practices, but it was probably like those of the two rural practitioners.
Graph 2
Josiah Bartlett’s average patient fees each year, and the average number of patients he saw daily, including house calls, each year, over the thirty-seven years spanned by his account books. Source: See text.
Bartlett saw patients most frequently in the autumn months, September through November, and least often in January and February (as determined by the mean number of patients seen each month during the thirty-seven years during which he kept the ledgers). This peak incidence of disease in the autumn was also felt in Portsmouth, where deaths were most numerous in the same months, but the fewest deaths occurred there in the spring, from March through June.11 However, many sporadically epidemic diseases with high morbidity have low mortality, and vice versa, factors which could well influence the value of this statistic (see, e.g., Table XV). Data for the other three physicians’ monthly practices were insufficient to permit making further comparisons.
table iii
Mean patient fees charged (although not necessarily collected) by four colonial New England physicians. Part of the large variation (as reflected in the Standard Deviations) can be attributed to the charges per mile superimposed on standard fees when making house calls outside each physician’s own town, and to the varying numbers of drugs prescribed by each physician.
|
Physician and period of his ledger (s) |
Fee per patient, in shillings (Mean ± s.d.) |
|
Josiah Bartlett, 1770–1787 |
1.9 + 0.5 |
|
Benjamin Rowe, Jr., 1785–1791 |
2.3 ± 0.4 |
|
William Aspinwall, 1782–1795 |
5.6 + 1.1 |
|
(after excluding deliveries*) |
(4.7 ± 0.9) |
|
David Townsend, 1784–1791 |
4.5 ± 0.9 |
|
(after excluding deliveries>*) |
(3–5 ± 0.7) |
Sources: See text.
* Both Aspinwall and Townsend charged twenty-eight shillings for attendance at a delivery; prenatal care seems not to have been included in that standard fee
table iv
Frequencies of bleeding, tooth extraction, application of dressings, opening abscesses, obstetrical deliveries, and other surgical procedures in four colonial New England medical practices. See Table V for a detailed list of the other operations performed by these physicians.
| Josiah Bartlett | ||||||||
|---|---|---|---|---|---|---|---|---|
| Quarter of ledger pages tallied | Benjamin Rowe, Jr. Jun. 1785–Jul. 1791 | William Aspinwall 1782–1795 | David Townsend 1784–1791 | |||||
| I | II | III | IV | Total | ||||
| Period of ledger(s)
All surgical treatments |
Jun. 1751–Jul. 1758 | Sep. 1758–Apr. 1764 | Jun. 1764–May 1770 | Aug. 1770–Dec. 1787 | Jun. 1751–Dec. 1787 | |||
|
among all patients |
11.7% |
25.3% |
20.2% |
12.8% |
17.6% |
22.7% |
5.6% |
13.6% |
|
Bleeding among |
||||||||
|
all patients |
4.4%* |
7.7%* |
7.3% |
2.9% |
5.8% |
5.2% |
0.8% |
0% |
|
% patients bled who also received drugs |
52.8% |
38.2% |
38.2% |
76.5% |
44.9% |
78.3% |
33.3% |
— |
|
Tooth extraction |
||||||||
|
among all patients |
2.4% |
6.1% |
4.6% |
3.4% |
4.1% |
5.3% |
0.6% |
1.0% |
|
Opening abscesses |
||||||||
|
among all patients |
0.8% |
1.5% |
1.4% |
0.5% |
1.1% |
2.2% |
0.3% |
0.3% |
|
0% |
0% |
0% |
0% |
0% |
0% |
2.1% |
1.9% |
|
|
% all patients who required dressings † |
3.8% |
9.1% |
6.3% |
5.4% |
6.1% |
9.3% |
0.6% |
9.8% |
|
% of these who also received drugs |
51.1% |
39.3% |
36.2% |
62.5% |
44.2% |
16.7% |
50.0% |
2.6% |
|
Other surgical procedures among all patients |
0.3% |
0.9% |
0.5% |
0.7% |
0.6% |
0.7% |
0.3% |
0.6% |
Sources: See text.
*Dr. Bartlett bled ten children by cutting the undersides of their tongues, all in only the first two quarters of the ledger pages sampled.
† Surgical and accidental wound dressings are collated here, because it was not possible to differentiate between them in most instances.
Graph 2 also shows that Dr. Bartlett’s professional fees increased at an average rate of about 2.4 shillings a year over the first thirteen years of his practice, until they fell suddenly, by ninety-five percent, in early 1765. Afterwards, he and Rowe charged similar fees, while their Boston colleagues charged about twice as much (Table III), presumably because the cost of living was greater in urban than in rural areas. During the entire period of his ledgers, Bartlett kept his accounts in pounds sterling, but he accepted Continental and, later, United States, money at current rates. For instance, on 31 December 1786, fifty dollars were credited to one patient’s account as four shillings and three pence.
The precipitous decline in Bartlett’s professional fees in early 1765 seems to be associated with the economic decline prevalent throughout the colonies. Most of this is attributable to the recession that followed the French and Indian War, along with Parliament’s ill-advised attempts to raise more revenue from the colonists. The Currency Act of 1764, which prohibited the printing of any more paper money in the colonies, and other acts regulating the colonial trades, probably combined with the acute money shortage, caused by the forcible removal of ready cash to England, to lower Bartlett’s fees. He could not have expected more from his patients, whose ability to pay seems to have been limited even in the best of times. Kingston was described, shortly after his death, as “chiefly a pine plain. It contains a scattered hamlet near the church. The houses throughout the town are indifferent. The soil is light and thin, the cultivation very ordinary, and the whole appearance of the country unpromising.”12
“Surgical” Treatments
Table IV shows the extents of non-drug treatments employed by the four New England physicians, treatments which, for convenience, will be called “surgical” here. Dr. Aspinwall used surgical techniques the least often, and Dr. Rowe the most often, although the ledgers provide no definitive clues that might explain the fourfold difference between the two practitioners. Presumably because Bartlett and Rowe were the only practitioners in their towns, they used surgical techniques more often than their colleagues in Boston, where opportunities for even primitive degrees of specialization were greater and more easily exploited.
The two rural physicians bled about five percent of their patients, while the two Boston doctors almost never did. In no instance was any one patient bled more than once for the same illness (i.e., within a year), but the amounts removed were not recorded in the ledgers. From one-third to three-fourths of the patients who were bled also received drugs at the same time, but there was no discernible association of specific drugs with bleeding. Bartlett bled women disproportionally more frequently (not tabulated) than expected from the proportion of women among his patients, but his reasons for doing so are not identifiable. On the other hand, both Rowe and Bartlett bled children in direct proportion to their numbers among those physicians’ practices (also see Table I), and Rowe also bled women in proportion to their numbers in his practice.
The Boston doctors extracted teeth much less often than did their counterparts in New Hampshire, where, presumably, physicians were called upon to render a greater diversity of professional services. None of the four physicians administered drugs to his dental extraction patients. In all four practices, the sex and age group of the dental patients were consistent with those of the entire practices. Tooth extractions may have been more common in America than elsewhere. Timothy Dwight remarked that “It is supposed that our teeth more generally decay at an untimely period than those of Europeans.”13
Again, the rural doctors opened abscesses more often than the city doctors did, but the rural doctors seem not to have delivered any babies, perhaps because the families of pregnant women provided whatever assistance was needed. There is no evidence of midwives practicing in Kingston or Kensington. Other kinds of nonmedical (i.e., non-drug) therapies were performed about equally frequently by the four physicians studied.
Numbers of nonmedical treatments (excluding bleeding and tooth extractions, for which see Table IV) provided by four colonial New England physicians.
| Number of times operation recorded in ledgers of: | ||||
|---|---|---|---|---|
| Bartlett | Rowe | Aspinwall | Townsend | |
|
Opening abscess on: |
||||
|
head, face, or neck |
10 |
2 |
||
|
hand, arm, axilla, or shoulder |
9 |
|||
|
foot, leg, or hip |
13 |
|||
|
trunk |
3 |
|||
|
breast, of women |
4 |
|||
|
unspecified sites |
2 |
27 |
5 |
|
|
Reduce fracture of: |
||||
|
arm or clavicle |
7 |
1 |
2 |
|
|
foot or leg |
2 |
2 |
2 |
|
|
jaw |
1 |
|||
|
Rasping foot bones |
1 |
|||
|
Insering seton, for wound drainage |
3 |
|||
|
Reduce dislocated finger or shoulder |
5 |
|||
|
Reduce hernia |
2 |
|||
|
Reduce hernia of rectum |
1 |
|||
|
Extract pin or splinter |
2 |
|||
|
Remove com from child’s ear |
1 |
|||
|
Remove mote [dust speck] from eye |
2 |
|||
|
Remove tumor, nature and site unspecified |
1 |
|||
|
Tapping of abdominal cavity |
5* |
|||
|
Smallpox inoculation |
2 |
|||
|
Obstetrical delivery |
30 |
15 |
||
Sources: See text.
*Dr. Rowe tapped his father, also a doctor, sixty-seven times, during which 2368 pounds of fluid were removed over twelve months in 1786–1787. The father survived another three years.
Dr. Aspinwall, in Boston, applied dressings to his patients, for whatever reasons, much less frequently than did the other three physicians. It is unlikely that this difference can be attributed to the availability of a “specialist,” but there may have been some other practical reason for it. The age and sex of patients who were dressed by all four physicians were in proportion to the age and sex groups of their entire patient populations, as shown in Table I. Drs. Rowe and Townsend, who used the most dressings, were also the least likely to give those same patients drugs at the same time.
The other surgical therapies the four doctors provided are listed in Table V. Although major operations such as couching for cataract (i.e., dislocating the opacified lens into the lower part of the eyeball) and amputations were being performed in Portsmouth and Boston at the same time, none of the four physicians seems to have done them. Smallpox inoculation was well known throughout New England, yet there is little evidence for it in the four ledgers. Aspinwall was regarded as a prominent inoculator, yet his ledgers show only two inoculations. However, inoculations were not usually given to private patients unless an epidemic threatened, so Aspinwall probably kept separate inoculation ledgers. Bartlett never even had himself inoculated until he went to Philadelphia in 1775, when Benjamin Rush immunized him for four pounds ten shillings. The ledger data confirm the memory of Bartlett’s son Levi, also a physician, who wrote that his father’s “feelings were too humane & tender to attempt operations in Surgery, or to shine as a Surgeon.” Because of this, it is likely that surgeons were called from Portsmouth or other towns when needed for major operations.14
The Medical Milieu of New Hampshire and Boston as Reflected in Mortality Data
Table VI shows crude death rates and ratios of deaths to births in colonial New Hampshire towns and in Boston. The data indicate that mortality rates were greater in the most densely populated areas, either when measured as crude death rates or when taken in conjunction with birth rates. In Boston, births just balanced deaths, whereas in rural New Hampshire each death was replaced by two births. (The high infant mortality rates would have lessened the actual ratio, but the infant mortality would have been even greater in Boston, resulting in greater net gains in the rural areas.) Throughout the eighteenth century, New Hampshire’s population was increasing more rapidly than that of all thirteen colonies combined, while the Massachusetts population was among the most slowly growing on the continent.15
table vi
Crude death rates and proportion of deaths to births in colonial New Hampshire towns and Boston in the eighteenth century.
| No. deaths per 1000 population | No. deaths per 100 births | |
|---|---|---|
|
Rochester, N.H. |
8.3 |
— |
|
Concord, N.H. |
10.3 |
— |
|
Kensington, N.H. (Dr. Rowe) |
10.4 |
— |
|
Andover, N.H. |
11.6 |
— |
|
Mason, N.H. |
12.8 |
43.5 |
|
Kingston, N.H. (Dr. Bartlett) |
14.5 |
— |
|
Amherst, N.H. |
14.8 |
— |
|
Hampton, N.H. |
— |
50.9 |
|
Newmarket, N.H. |
— |
58.4 |
|
Portsmouth, N.H. |
18.1 |
46.2 |
|
Boston, Mass. |
36.6 |
98.6–117.2 |
Sources: Daniel Adams, ed., Medical and Agricultural Register, 1 (1806–1807), 284–285; Jeremy Belknap, History of New-Hampshire, 2nd ed., 3 v. (Boston, 1813), III, 179–184; J. P. Brissot de Warville, New Travels in the United States of America 1788, trans. Mara Soceanu Vamos and Durand Echeverria (Cambridge, Mass., 1964), 288; J. Farmer and J. B. Moore, Collections, Topographical,... New Hampshire, 3 v. (Concord, 1822), I, 24, 80–83; Ora Pearson, “Bill of Mortality for Kingston, N.H.,” Collections of the New Hampshire Historical Society, 5 (1837), 250–252; Lyman Spalding and Richard Thurston, Bills of Mortality for Portsmouth, New Hampshire (1801–1811, 1818–1820), in Boston Medical Library; J. Worth Estes, “‘As Healthy a Place as Any in America’: Revolutionary Portsmouth, N.H.,” Bulletin of the History of Medicine, 50 (1976), 536–552; Jabez Dow, Bill of Mortality for Kensington, N.H. (Dover, N.H., 1802).
Table VII shows that there were more deaths in Josiah Bartlett’s Kingston than in Benjamin Rowe’s Kensington during the middle six decades of the eighteenth century, when Kingston was presumably a little larger. Not until the last two decades did the numbers of deaths in the two towns become approximately equal, as were their populations by then. There is no reason to believe that Kensington’s patients received medical care that was substantially different from that offered in Kingston; the throat distemper epidemic which affected much of New Hampshire in the first half of the century was responsible for many more deaths in Kingston than in Kensington.
table vii
Mean annual number of deaths (with Standard Deviations) during decennial periods in Kingston and Kensington, New Hampshire, throughout the eighteenth century. See Table II for the populations of the two towns.
| Years | Kingston | Mean + s.d. annual number of deaths in Kensington |
|---|---|---|
|
1720–1730 |
8.6 + 7.9 |
— |
|
1731–1740 |
22.7 + 29.3* |
3.7 ± 2.1 |
|
1741–1750 |
19.1 ± 9.8 |
9.2 ± 8.5 |
|
1751–1760 |
17.8 + 8.6 |
12.0 + 8.3 |
|
1761–1770 |
— |
7.2 ± 3.1 |
|
1771–1780 |
10.5 + 7.3 |
7.1 ± 2.4 |
|
1781–1790 |
9.3 + 3.2 |
8.9 ± 5.6 |
|
1791–1800 |
9.2 ± 4.2 |
8.7 + 4.3 |
Sources: Ora Pearson, “Bill of Mortality for Kingston, N.H.,” New Hampshire Historical Society Collections, 5 (1837), 250–252; Jabez Dow, Bill of Mortality for Kensington, N.H. (Dover, N.H., 1802).
* When the deaths attributed to the 1735 epidemic of throat distemper are subtracted, this value falls to 13.9 ± 9.6.
table viii
Recorded causes of death in colonial New Hampshire and Boston.
Sources: Jeremy Belknap, History of New-Hampshire, 2nd ed., 3 v. (Boston, 1813), III, 179–187; Jabez Dow, Bill of Mortality for Kensington, N.H. (Dover, N.H., 1802); Lyman Spalding and Richard Thurston, Bills of Mortality for Portsmouth, New Hampshire (1801–1811, 1818–1820), in Boston Medical Library; Lemuel Shattuck, The Vital Statistics of Boston (Philadelphia, 1841).
During the years of Bartlett’s ledgers for which data are available, the people of Kingston suffered an average of about thirteen deaths per year, slightly less than for the entire period. Rowe’s entire practice spanned the last three decades of the eighteenth century; during the few years covered in his ledger, the mean annual number of deaths in Kensington was about nine, just slightly more than that for his entire career.16
The reported causes of death in Hampton and Dover, where some of Bartlett’s patients lived, in Kensington, where most of Rowe’s patients lived, and in Portsmouth and Boston are listed in Table VIII. Although it is notoriously difficult to equate eighteenth-century diagnoses with those in use today, the earlier diagnoses can be categorized into certain general classes. For instance, infectious diseases, especially among children, were the leading causes of death in our four physicians’ practices. Of these, consumption, most cases of which were probably caused by the tubercle bacillus, was most conspicuous. Some diagnoses, such as convulsions, fever, cough, diarrhea, dysentery, and putrid fever were too nonspecific to be easily interpretable today. But other diseases, such as bilious colic, measles, scarlet fever, smallpox, whooping cough, and perhaps childbed fever are less likely to be misunderstood in terms of twentieth-century concepts of their etiology.
In general, the data in Table VIII show considerable uniformity among the attending physicians’ diagnostic standards. For the New Hampshire towns at least, and probably in Portsmouth and Boston, the diagnoses given in their bills of mortality were originally made by doctors in those communities, not by nonprofessionals (like those who had contributed to the earlier London bills, for instance). The one major difference is for the throat distemper, which appeared from 1735 to 1740 in Kingston and spread to many rural New England towns, while inflicting relatively little damage on the large seaport towns. Probably a combination of diphtheria and scarlet fever, the throat distemper’s effects are still seen in the Kingston cemetery, in the midst of which is a large swath of small children’s headstones, most of them dated 1735 (at which time Josiah Bartlett was only six years old).17 It is unlikely that even the few deaths attributed to the throat distemper in Portsmouth and Boston after the turn of the century were, in fact, caused by the same combination of bacteria that had attacked rural New England many years earlier.
In all the ledger pages sampled in this study, only three deaths were noted, all in William Aspinwall’s Boston practice. Of these, the cause was given for only one, “in childbirth.” Both Aspinwall and Bartlett noted that a single patient had measles; presumably both patients survived.
Because the Kensington bills of mortality are given by year, it is possible to determine just which patients died during Benjamin Rowe’s practice in that town and, consequently, which diagnoses he must have made both throughout his career and during the period of his ledger. Mortality among infants dropped from sixteen percent of Kensington deaths before Rowe began his practice to eleven percent afterwards (although, as noted earlier, Rowe seems to have few pediatric patients), while deaths attributed to consumption climbed from five percent to eighteen percent (probably as the town grew in population), and those to dropsy from three percent to five percent. Otherwise, Rowe’s diagnoses of causes of death do not differ remarkably from those made by his father, who had had the entire practice of Kensington before the son opened his own practice in adjacent East Kensington.
Pride in local longevity was endemic throughout early America, an early form of chauvinism that was consistent with the very concept of a New World. Although the Kingston bills of mortality list no diagnoses, names and ages are given for persons who died at ages greater than ninety. Of sixteen nonagenarians dying in Kingston between 1751, when Bartlett began his practice, and 1810 (only five were men), virtually all were or had been his patients, as can be determined from his ledgers.
Life expectancies, in years, for colonial New Hampshire towns and Boston. The total life expectancy experience is measured as the area under the life expectancy curve, here compared with that for Portsmouth as the standard.
| Dover, | Rochester, | Hampton, | Concord | Portsmouth, | Boston, | |
|---|---|---|---|---|---|---|
| At age | 10 yrs., 18th cen. | 1776–1822 | 1735–1792 | 1798–1821 | 1801–1820 | 1811–1820 |
|
0–5 |
— |
33 |
20 |
29 |
32 |
28 |
|
6–10 |
— |
44 |
24 |
42 |
41 |
36 |
|
11–20 |
— |
43 |
43 |
40 |
37 |
33 |
|
21–30 |
— |
38 |
39 |
34 |
33 |
26 |
|
31–40 |
35 |
33 |
37 |
30 |
27 |
22 |
|
41–50 |
29 |
28 |
31 |
26 |
23 |
19 |
|
51–60 |
23 |
23 |
24 |
21 |
18 |
17 |
|
61–70 |
15 |
17 |
17 |
15 |
14 |
13 |
|
71–80 |
10 |
11 |
11 |
12 |
9 |
9 |
|
81–90 |
7 |
7 |
8 |
7 |
6 |
6 |
|
Total life expectancy experience |
121% |
117% |
115% |
109% |
100% |
84% |
Sources: Jeremy Belknap, History of New-Hampshire, 2nd ed., 3 v. (Boston, 1813), III, 178–187; J. P. Brissot de Warville, New Travels in the United States of America 1788, trans. Mara Soceanu Vamos and Durand Echeverria (Cambridge, Mass., 1964), 288; J. Farmer and J. B. Moore, Collections, Topographical,. . . New Hampshire, 3 v. (Concord, 1822), I, 24, 81–83; Lyman Spalding and Richard Thurston, Bills of Mortality for Portsmouth, New Hampshire (1801–1811, 1818–1820), in Boston Medical Library; Lemuel Shattuck, The Vital Statistics of Boston (Philadelphia, 1841); “Bill of Mortality for Rochester, N.H.,” Collections of the New Hampshire Historical Society, 1 (1824), 283–284; J. Worth Estes, “‘As Healthy a Place as Any in America’: Revolutionary Portsmouth, N.H.,” Bulletin of the History of Medicine, 50 (1976), 536–552.
The crude death rate and consumption mortality data (in Tables VI and VIII) are again reflected in life expectancies in four rural New Hampshire towns, Portsmouth, and Boston, as seen in Table IX. Because there were no additions to physicians’ therapeutic tools in the last decade of the eighteenth century that might have substantially altered the death rates or longevity for entire populations, the data for the two larger communities can be considered to reflect at least the same situation which must have been found there throughout the last half of the century.
The data in Table IX, like those in Tables VI and VIII, support the hypothesis, well known to contemporary writers such as Malthus, that mortality and presumably morbidity were proportional to population density. That is, inhabitants of the smallest and least heavily populated communities could expect to live longer than those in the more populous cities and towns. Aspinwall and Townsend, then, would have had fewer older patients, and would have seen higher morbidity and mortality rates among their patients than would Bartlett and Rowe.
Drug Therapies
About ten percent of patients in the four colonial New England practices received no drugs at all. Dr. Rowe used fewer drugs than his three colleagues, and Dr. Townsend was the most likely to administer no therapy of any kind at all. Bartlett gave “Directions” for self-care to 5.3% of his patients, Rowe to 0.5%, Aspinwall to 1.0%, and Townsend to 0.1%. Bartlett “advised” other physicians as to the care of their patients four times, and Aspinwall twice. Paid professional consultations, therefore, seem to have been as rare in the city as in the country, but Bartlett may have distinguished himself for the number of instructions to patients for their own care.
Colonial physicians seem not to have practiced polypharmacy to any great extent, as seen in Table X. The average number of drugs prescribed for all patients, including “surgical” patients, ranged from about 1.0, in Boston, to about 1.5 in rural New Hampshire. The median number of drugs administered to nonsurgical (i.e., “medical”) patients was even lower, ranging from about 0.5 in Boston to a little over 1.0 in New Hampshire. Bartlett prescribed more drugs in the late 1760’s than during the rest of his practice, but the reason is not now obvious. In general, the Boston physicians used fewer drugs than the country doctors, but multiple drug use was nowhere common. In fact, the Appendix shows that even those drugs that had more than one ingredient were few, and in the vast majority the other ingredients were not even then thought to be active drug principles.
Numbers of drugs prescribed for their patients by four colonial New England physicians.
|
Josiah Bartlett |
||||||||
|
Quarter of ledger pages tallied |
Benjamin Rowe, Jr. Jun. 1785–Jul. 1791 |
William Aspinwall 1782–1795 |
David Townsed 1784–1791 |
|||||
|
I |
II |
III |
IV |
Total |
||||
|
Period of ledger (s) |
Jun. 1751–Jul 1758 |
Sep. 1758–Apr. 1764 |
Jun. 1764–May 1770 |
Aug. 1770–Dec. 1787 |
Jun. 1751–Dec. 1787 |
|||
|
Number of drugs prescribed for all patients |
1895 |
1701 |
1953 |
1017 |
6566 |
1602 |
1116 |
618 |
|
% all patients receiving drug therapy only |
94.3% |
92.7% |
93.7% |
96.2% |
93.8% |
75.8% |
94.9% |
89.5% |
|
Fraction of patients* given: |
||||||||
|
No treatment |
7.7% |
5.2% |
7.4% |
11.2% |
7.5% |
6.5% |
— |
31.3% |
|
One drug |
29.3% |
31.2% |
22.2% |
31.3% |
28.4% |
35.5% |
— |
43.3% |
|
Two drugs |
25.1% |
19.1% |
18.9% |
22.7% |
21.6% |
24.8% |
12.2% |
|
|
Three drugs |
13.3% |
11.0% |
14.2% |
10.9% |
12.5% |
10.7% |
— |
2.2% |
|
Four drugs |
4.6% |
8.2% |
7.9% |
7.0% |
6.8% |
3.6% |
0.5% |
|
|
Five or more drugs |
2.2% |
5.2% |
11.6% |
4.3% |
5.7% |
1.2% |
— |
0.0% |
|
Number of drugs prescribed |
||||||||
|
per patient, all patients |
1.5 |
1.6 |
2.0 |
1.6 |
1.7 |
1.4 |
0.8 |
1.0 |
|
Median number of drugs prescribed for non-surgical patients |
1.2 |
1.2 |
1.5 |
1.1 |
1.2 |
1.0 |
— |
0.5 |
Sources: See text.
* Excluding patients who received only surgical treatments (given in Table IV).
Drugs administered by four colonial New England physicians, grouped according to the classification of James Thacher (for which see the Appendix), and arranged by decreasing frequency of Josiah Bartlett’s usage of each drug class. Within the classes, drugs are listed alphabetically after those of unknown composition but with names which necessitate their inclusion in the class. Individual drugs are identified in the Appendix. Each drug was assigned to the first drug class given for it by Thacher; when he ascribed other attributes to any drug, its secondary class assignments are given in square brackets in this Table. Alternative drug names used by any of the four physicians are given in parentheses.
| % all drugs administered by Doctors: | ||||
|---|---|---|---|---|
| Bartlett | Rowe | Aspinwall | Townsend | |
| In years | 1751–87 | 1785–91 | 1782–95 | 1784–91 |
| Fraction of ledger pages sampled | 10% | 10% | 10% | 30% |
| Total number of drugs administered | 6566 | 1602 | 1116 | 618 |
DRUGS AND DRUG CLASSES [other classes to which drugs also assigned by Thacher]
|
CATHARTICS |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Aperients subclass | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
bal polychrestum |
0.47 |
0.69 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
de mellilot [Expectorant] |
0.70 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
oxymel [Expectorant] |
0 |
1.94 |
0.09 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
salop [Diuretic, Diaphoretic] |
0.11 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
sambucus |
0.02 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
laxative, unspecified |
0 |
0 |
0 |
0.49 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
balsam of sulphur |
0.37 |
0.69 |
0.09 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
gum manna |
0.30 |
0.75 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
lenitive electuary |
0 |
0 |
0.09 |
0.16 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ol oliva |
0.17 |
1.06 |
0.09 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
raisins |
0 |
0.06 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
saline cathartic |
0 |
0 |
1.25 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
spirits of mindererus [Diaphoretic] |
0.12 |
0 |
24.91 |
0.16 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Purgatives subclass |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
cathartic pills/powder, unspecified |
3.79 |
3.68 |
20.34 |
12.62 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
cathartic digestive, unspecified |
0 |
0.37 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
cathartic enema, unspecified |
0.05 |
0.06 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
physick, unspecified |
0.09 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
low cathartic |
0 |
0 |
0 |
0.16 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
haust[us] cathartic [us] |
0 |
0 |
0 |
1.46 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
purgative apozemata |
0.62 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
aloes |
0.03 |
0 |
0.09 |
0.32 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
buckthorn, syrup of [Tonic] |
0 |
0.06 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
calomel (= cathartic dulcis) |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
[Anthelminthic, Diuretic] |
0.46 |
0 |
0.27 |
2.59 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
essence veneris |
0.03 |
0.19 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
mercurial pill |
0 |
0.06 |
0.63 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
pill unique |
0 |
2.43 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
van swieten’s antivenereal |
0.02 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Bartlett |
Rowe |
Aspinwall |
Townsend |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
3.53 |
2.68 |
0.45 |
0.81 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
cremor tartar [Diuretic] |
0.87 |
0.69 |
0.27 |
0.16 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
elixir proprietatis |
1.11 |
2.18 |
0.27 |
0.32 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
elixir salutis |
0.78 |
0.62 |
0 |
0.65 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
sal mirabile glaube [Diuretic] |
0.06 |
1.94 |
0.18 |
0.16 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
jalap |
0.08 |
0.31 |
0.54 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
helleborus niger |
0.26 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
hiera picra |
2.27 |
3.12 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
nicotinic cathartic |
0 |
0 |
0.09 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
rhei [Astringent] |
2.51 |
3.68 |
2.15 |
0.97 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
rufus’ pill |
0 |
0 |
0 |
0.32 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
sal catharticus amarus |
0.58 |
0.06 |
0 |
0.49 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
scammony |
0 |
0 |
0.09 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
sennae, foliae [Diuretic] |
0.23 |
0.12 |
0.27 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
tinctura sacra [Tonic] |
0.37 |
0 |
0.18 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ALL CATHARTICS |
19.98 |
27.47 |
52.33 |
21.84 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
NARCOTICS |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
camphor, elixir [Antispasmodic] |
12.35 |
0.50 |
1.52 |
1.29 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
camphor, gum (applied topically) |
1.07 |
0.94 |
0.27 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
lactuca |
0 |
0 |
0.09 |
0.16 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
nicotinic unguent [Emetic, Cathartic] |
0.44 |
0 |
0.18 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
opium |
0.08 |
0.06 |
0.09 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
anodyne balsam |
2.80 |
0.87 |
3.94 |
2.43 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
0.09 |
0 |
0 |
0.65 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
diacodium |
0.02 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
elixir asthmaticus |
0.58 |
0 |
1.97 |
0.32 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
liquid laudanum |
0.05 |
0.06 |
0.09 |
0.16 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
paregoric elixir |
0.14 |
2.37 |
0.36 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
thebaic tincture |
0 |
0 |
0.18 |
0.16 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
theriac |
0.21 |
0 |
0.09 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ALL NARCOTICS |
17.82 |
4.81 |
8.78 |
5.18 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
TONICS |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Stomachics subclass |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
stomachic/digestive pills (=tincture amara) |
0 |
1.56 |
0.18 |
0.32 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
stomachic emplastrum |
0 |
0.25 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
peptic pill/powder, unspecified |
0.37 |
0.44 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
anise, ol/semina |
0.97 |
0.56 |
0.27 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
bitters |
2.53 |
0 |
0.09 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
carminative |
0.43 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
chamomile, florae [Diaphoretic] |
0.49 |
0.25 |
0.54 |
0.16 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
cinnamon, ol/cortex (=aromatic tincture) |
0.29 |
0.06 |
0 |
0.32 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
colombo, tincture of |
0 |
0 |
0 |
0.65 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
elixir/ol vitriol (=acid drops) |
0.38 |
1.62 |
0.18 |
0.16 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
vitriol romanum |
0.35 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
galingale |
0.03 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
guaiac, gum/tincture [Diuretic, Diaphoretic] |
0.69 |
1.06 |
0.54 |
0.16 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
hippocondrial infusion |
0.02 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Rowe |
Aspinwall |
Townsend |
||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
myrrha, tincture [Diaphoretic, Expectorant] |
0.24 |
0.87 |
0.09 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
nux moschata mare |
0.02 |
0 |
0 |
0.16 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
mentha, ol |
0.05 |
0.06 |
0.09 |
0.16 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
pulegi, ol |
0.05 |
0.06 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
quassia infusion |
0 |
0 |
0 |
0.32 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
saline [Cathartic] |
0.02 |
0 |
0.09 |
0.32 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
serpentina, radix [Diaphoretic] |
2.56 |
1.87 |
1.79 |
1.46 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
spirits of wine |
0.05 |
0 |
0 |
0.16 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
uva ursi |
0 |
0.06 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
| General Tonics subclass | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
baricis [Diaphoretic, Diuretic] |
0.02 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
capivi, balsam of |
0.29 |
1.19 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
carbonas ammoniae (=spirits of ammonia) |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
[Diaphoretic] |
0 |
0.06 |
0 |
1.46 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
cardiac drops |
0.02 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
cordial julep |
0.12 |
0.12 |
0.09 |
0.97 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
curcuma, radix |
0.06 |
0.37 |
0.09 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
emplastrum hemloc |
0 |
0.12 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
gentiana, radix |
0.11 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
lavender, compound spirits of |
2.00 |
0.75 |
0.81 |
0.65 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
stoughton’s elixir/tincture/drops |
3.62 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
succinum, ol [Cathartic] |
0.43 |
0.06 |
0 |
0.49 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
succinum, sal [Cathartic] |
0.32 |
0.94 |
0 |
0.65 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
0.27 |
0 |
0 |
1.13 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ALL TONICS |
16.75 |
12.36 |
4.84 |
9.71 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ASTRINGENTS |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
restringent |
0.40 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
alumen |
0.03 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
aqua calcis [Antacid] |
0.03 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
areci, liniment |
0.02 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
bole [?armeniac] |
0 |
0 |
0.09 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
calybeate |
1.34 |
1.44 |
0.27 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
cascarilla (=cortex eleutheria) |
0 |
0.12 |
4.84 |
0.49 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
cerralina |
0 |
0.06 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
contrayerva, radix [Diaphoretic] |
0.15 |
0.37 |
0.54 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
cortex peruviana, powder/decoctionz |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
infusion / tincture |
2.48 |
3.93 |
2.51 |
11.00 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
alex[ipharmical] tincture |
4.55 |
6.74 |
0.09 |
0.16 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
cortex pulves rubrum |
0 |
0 |
0 |
2.10 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
huxham’s tincture |
0 |
0 |
0 |
0.49 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
tormentilla |
0 |
0 |
0.09 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ALL ASTRINGENTS |
9.00 |
12.67 |
8.42 |
14.24 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ANTISPASMODICS |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
antispasmodic bolus, unspecified |
0 |
0 |
0.81 |
0.32 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
antihysteric plaster [Expectorant] |
0.99 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
gum ammoniac [Expectorant] |
0.03 |
0.94 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Rowe |
Aspinwall |
Townsend |
||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
gum fetida/assa fetida [Expectorant] |
0.47 |
0.19 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
fetid tincture/powder/pill [Expectorant] |
0.75 |
0.37 |
0.63 |
0.32 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
gum galbanum |
0 |
0.37 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
hungary water |
0.02 |
0.37 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
valerian, radix |
0.53 |
3.81 |
0.18 |
0.65 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
volatile drops |
2.99 |
1.06 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ALL ANTISPASMODICS |
5.77 |
7.12 |
1.61 |
1.29 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
EPISPASTICS AND RUBEFACIENTS |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
epispastic ointments |
2.63 |
5.06 |
2.96 |
1.46 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
cantharides [Diuretic] |
2.22 |
0.81 |
0.09 |
0.49 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
balsam abietis |
0.05 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
prunella, sal |
0.02 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ALL EPISPASTICS |
4.92 |
5.87 |
3.05 |
1.94 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
EMETICS |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
emetic, unspecified (?Lobelia inflata) |
1.31 |
5.06 |
0 |
7.61 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
antimony, essence/powder/crocus of |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
[Diaphoretic] |
0.09 |
0 |
0.99 |
6.31 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
balsam flavus (=turpeth mineralis) [Errhine] |
1.83 |
0 |
0.09 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ipecacuanha [Diaphoretic] |
0.03 |
0.44 |
0.36 |
0.49 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
tartar emetic [Cathartic, Diaphoretic] |
0.02 |
0.06 |
0.36 |
0.32 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
turmeric [Cathartic] |
0 |
0 |
0.09 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
vitriol alba |
0.06 |
0.12 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
0.29 |
0 |
0 |
0 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ALL EMETICS |
3.63 |
5.68 |
1.89 |
14.73 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
REFRIGERANTS |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
cortex aurantium |
0.09 |
0 |
0.09 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
dulcified spirit of nitre [Tonic, Diaphoretic, |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Diuretic] |
2.47 |
0.25 |
0.45 |
1.29 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
hord [eum distichon] |
0 |
0 |
0 |
0.32 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
sal nitre [Diuretic] |
0.50 |
2.56 |
0.36 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
unguent alba |
0.18 |
0.06 |
0 |
1.46 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ALL REFRIGERANTS |
3.24 |
2.87 |
0.90 |
3.07 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
DEMULCENTS |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
gum arabic |
0.12 |
0.31 |
0.09 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
liquorice (=glycerrhiza) |
2.35 |
0.25 |
0.36 |
0.49 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
spermaceti |
0.75 |
0.87 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ALL DEMULCENTS |
3.21 |
1.44 |
0.45 |
0.49 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
DIAPHORETICS |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
diaphoretic/sudorific powder, unspecified |
0.08 |
1.62 |
0 |
0.16 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
pectoral powder/decoction/balsam, unspecified |
0.38 |
0.56 |
0.81 |
0.49 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
antirheumatic pill (?Dover’s) |
0 |
0 |
0.18 |
0.65 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
benzoin, florae |
0.15 |
0.50 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
sulfur, flowers of/crude |
1.34 |
0 |
0.27 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
prickly ash |
0 |
0.19 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Rowe |
Aspinwall |
Townsend |
||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
dr. bateman’s pectoral drops |
0.06 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ALL DIAPHORETICS |
2.01 |
2.87 |
1.26 |
1.30 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
DIURETICS |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
diuretic salt/powder/pill, unspecified |
0.21 |
0 |
0 |
0.65 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
pisser(?) |
0 |
0 |
0.09 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
borax [Emmenagogue, Topical] |
0.17 |
0 |
0 |
0.16 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ol terebinth (= venice turpentine) |
0.70 |
0.50 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
sal tartari (=sal absinthum) |
0.11 |
0.69 |
0.45 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
squills |
0.29 |
1.06 |
0.72 |
1.94 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ALL DIURETICS |
1.48 |
2.25 |
1.25 |
2.75 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ANTHELMINTICS |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
vermifuge, unspecified |
0.30 |
0 |
0.09 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ethiops mineralis |
0.53 |
0.44 |
0.54 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
pink root [Cathartic, Emetic] |
0.03 |
0.12 |
0.09 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
wormseed |
0 |
0.06 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ALL ANTHELMINTICS |
0.87 |
0.62 |
0.72 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ESCHAROTICS |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
caustic |
0 |
0.31 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
mercuric precipitate rubrum |
0.40 |
0.75 |
0 |
0.16 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
unguent egyptiae |
0.02 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
verdegris (=bal virid) |
0.18 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
0.06 |
0 |
0 |
0 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ALL ESCHAROTICS |
0.65 |
1.06 |
0 |
0.16 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ANTACIDS |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
magnesia alba [Cathartic] |
0.29 |
0.81 |
0.09 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
sal carbonas calcis (=corral) |
0.02 |
1.31 |
0.09 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ALL ANTACIDS |
0.30 |
2.12 |
0.18 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
SIALOGOGUES |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
cinnabar nativa |
0.18 |
0.50 |
0.18 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ALL SIALOGOGUES |
0.18 |
0.50 |
0.18 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
EMMENAGOGUES |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
emmenagogue/uterine elixir, unspecified |
0.05 |
0.06 |
0 |
0.16 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
juniper [Aperient, Diaphoretic] |
0.03 |
0.25 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ALLEMMENAGOGUES |
0.08 |
0.31 |
0 |
0.16 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
LITHONTRIPTICS |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
alkaline salt |
0.03 |
0 |
0.09 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ALL LITHONTRIPTICS |
0.03 |
0 |
0.09 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
EXPECTORANTS |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
expectorant mixture, unspecified |
0 |
0 |
0 |
1.46 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
lac ammoniaci |
0 |
0.50 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
traumatic balsam |
0 |
0.25 |
0 |
0.32 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ALL EXPECTORANTS |
0 |
0.75 |
0 |
1.78 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Rowe |
Aspinwall |
Townsend |
||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ERRHINES (Note secondary errhinc designations under other classes) |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
cephalic [? snuff] (?) |
0 |
0 |
0.09 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ALL ERRHINES |
0 |
0 |
0.09 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
DILUENTS |
0 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
EMOLLIENTS, external |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
unguent / liniment / embrocatio / lotio / salve, unspecified |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
0.02 |
0.25 |
0.45 |
2.75 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
balsam lucatelli |
0.14 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
basilicon ointment |
0.85 |
2.25 |
0.36 |
0.32 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
elixir supplanttva |
0 |
0.06 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
gum emplastrum, unspecified |
0 |
0.37 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ichthyocolla |
0.09 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
liniment, cerate (=calamine) |
0 |
0.44 |
0.54 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
unguent for burns |
0.02 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
unguent/embrocatio cortex peruviana |
0 |
0 |
0 |
0.32 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
unguent cosmetic |
0 |
0 |
0 |
0.16 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
unguent/embrocatio dialthea |
0.29 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
unguent emollient/molei |
0.91 |
1.12 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
unguent lectisternium |
0 |
0 |
0 |
2.27 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
unguent nervinum |
0.21 |
0.31 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
unguent tutiae/ophthalmic |
0.20 |
0 |
0 |
1.29 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
0.05 |
0 |
0 |
0 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ALL EMOLLIENTS |
2.77 |
4.81 |
1.34 |
7.12 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
PLASTERS and Other Non-Emollient External Medications |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
plaster, unspecified |
0.79 |
0.56 |
0.18 |
0.16 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
plaster, strengthening |
0.23 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
plaster, umbel |
0.08 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
balsam rubrum |
0.02 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
blisters (=tincture vessicativum) |
0.02 |
0 |
0 |
0.65 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
cerusse |
0.02 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
compress |
0 |
0 |
0.09 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
emplastrum deran(?) |
0.09 |
0.19 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
emplastrum diachylon |
0.17 |
0.87 |
0.09 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
emplastrum diapalma |
0.81 |
0.44 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
emplastrum dorsal |
0 |
0.87 |
0 |
0.16 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
emplastrum paracelsum |
0.06 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
liniment de minio negri |
0.05 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ungent dessicativum rubrum |
0.05 |
0 |
0.09 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
unguent mercuriale |
0.02 |
0 |
0.18 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ungent morraine [murrain] |
0 |
0.06 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
unguent neapolitan |
0.40 |
0.06 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
unguent saturnine (= vegeto-mineral water) |
0 |
0 |
0 |
3.88 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ALL PLASTERS |
2.77 |
3.06 |
0.63 |
4.85 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Rowe |
Aspinwall |
Townsend |
||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
AGENTS OF UNKNOWN COMPOSITION OR UNASSIGNABLE |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
IN THACHER’S CLASSIFICATION |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
“medicine” |
0 |
0.06 |
9.05 |
0.97 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
pill/powder/ebol/essence, unspecified |
0.46 |
0 |
1.25 |
1.78 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
absorbent |
1.54 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
alterative |
0 |
0 |
0 |
0.32 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
anticonvulsant |
0.02 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
antiemetic |
0.43 |
0 |
0 |
0.16 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
antifebritic/febrifuge |
1.58 |
0.31 |
0.09 |
1.78 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
anti-icteric |
0 |
0 |
0 |
1.46 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
antiphlogistic |
0 |
0 |
0.09 |
0.32 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
balsam mixture |
0.09 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
bryonia |
0 |
0 |
0 |
0.16 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
capers |
0 |
0 |
0.09 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
chart (?charcoal) |
0 |
0 |
0.90 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
diet drink (often Liquorice) |
0.05 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
elapi (=phosphate mixture), for rickets |
0 |
0.19 |
0 |
0.65 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
elixir warner |
0 |
0 |
0 |
0.16 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
fenugreek |
0.02 |
0.06 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
gargle |
0.05 |
0 |
0.09 |
0.97 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ol hedera |
0.02 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
perce |
0.06 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
pill sapo |
0 |
0 |
0 |
0.32 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
0.09 |
0.06 |
0 |
0 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
sal pourdre |
0.06 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
saxifrage |
0.05 |
0 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
syrup of balsam |
0.03 |
0.12 |
0 |
0 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Illegible or undecipherable |
0 |
0.56 |
0.54 |
0.32 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ALL UNKNOWN, UNASSIGNED |
4.52 |
1.37 |
12.10 |
9.39 |
||||||||||||||||||||||||||||||||||||||||||||||||||||
Sources: Frank C. Mevers, ed., Microfilm Edition of the Papers of Josiah Bartlett (1729–1795), 7 rolls (Concord, N.H., 1976), rolls 6 and 7, every tenth frame from frames 3663 to 4562; every tenth double page of the ledger of Dr. Benjamin Rowe, Jr., a 10% random sampling of well-filled legible pages of the ledger of Dr. William Aspinwall, and a 30% sampling of similar pages of the ledger of Dr. David Townsend, all in the Boston Medical Library, James Thacher, The American New Dispensatory (Boston, 1810), passim; P. S. Brown, “Medicines Advertised in Eighteenth-Century Bath Newspapers,” Medical History, 20 (1976), 152–168; James McKittrick Adair, Medical Cautions ... (London, 1787), 85; A. C. Wootton, Chronicles of Pharmacy, 2 v. in 1 (1910; rpt. ed., Boston, 1971); J. Worth Estes, “John Jones’s Mysteries of Opium Revcal’d (1701): Key to Historical Opiates,” Journal of the History of Medicine and Allied Sciences, 34 (1979), 200–209; The Merck Index, 7th ed. (Rahway, N.J., 1960); John Woodall, The Surgion’s Mate (London, 1617).
Presumed active ingredients, as listed by James Thacher, of drugs administered by four colonial New England physicians. Modern names for chemical compounds, and for plant and animal species, genera, and families are used. Because some drugs had more than one active ingredient, and because some drugs listed in Table XI had no active ingredients, according to their eighteenth-century users, the sums of all ingredients used by each practitioner do not add up to 100%. The agents listed are arranged by decreasing frequency of Josiah Bartlett’s use of each.
| In % of drugs prescribed or dispensed by: | ||||
|---|---|---|---|---|
| Active Ingredient | Bartlett | Rowe | Aspinwall Townsend | |
|
*Camphor (Cinnamonum camphora) |
14.25 |
3.81 |
4.21 |
1.61 |
|
*Peruvian Bark (Cinchona spp.) |
7.04 |
10.67 |
2.60 |
13.75 |
|
*Cantharides (Lytta vesicatoria) |
4.87 |
5.87 |
2.96 |
1.95 |
|
*Rhubarb (Rheum palmatum) |
4.07 |
3.86 |
2.47 |
0.97 |
|
*Opium (Papaver somniferum) |
3.96 |
3.37 |
6.72 |
3.72 |
|
Aloes (Aloe spp.) |
3.80 |
5.30 |
25.45 |
1.44 |
|
Castor Oil (Ricinus communis) |
3.53 |
2.68 |
0.45 |
0.81 |
|
*Mercury and Mercurial Salts |
3.37 |
4.31 |
1.26 |
2.75 |
|
*Cajeput (Melaleuca leucadendron) |
2.99 |
1.06 |
0 |
0 |
|
Virginia Snakeroot (Aristolochia serpentaria) |
2.56 |
1.87 |
1.79 |
1.46 |
|
Bitters (Cusparia angustura) |
2.53 |
0 |
0.09 |
0 |
|
Nitric and Nitrous Acids |
2.47 |
0.25 |
0.45 |
1.29 |
|
Liquorice (Glycerrhiza glabra) |
2.40 |
0.25 |
0.45 |
0.65 |
|
*Asafetida (Ferula spp.) |
2.21 |
0.56 |
0.63 |
0.32 |
|
2.00 |
1.12 |
0.81 |
0.65 |
|
|
Lavender (Lavandula officinalis) |
2.00 |
0.75 |
0.81 |
0.65 |
|
Lead Salts |
1.56 |
1.37 |
0.18 |
6.63 |
|
*Myrrh (Commiphora spp.) |
1.35 |
3.05 |
0.36 |
0.36 |
|
Iron Tartrates (probably really Oxides) |
1.34 |
1.44 |
0.27 |
0 |
|
Emetic [perhaps Emetic Weed, Lobelia inflata] |
1.31 |
5.06 |
0 |
7.61 |
|
*Anise (Pimpinella anisum) |
1.03 |
0.56 |
0.27 |
0 |
|
† Senna (Cassia spp.) |
1.01 |
0.74 |
0.36 |
0.81 |
|
Potassium Bitartrate |
0.87 |
0.69 |
0.27 |
0.16 |
|
*Jalap (Exogonium purga) |
0.86 |
0.93 |
0.54 |
0.65 |
|
Lard & Other Animal Fats |
0.85 |
2.75 |
0.36 |
0.32 |
|
*Palm Oil (Elaeis guineensis) |
0.81 |
0.44 |
0 |
0 |
|
*Amber Distillation Products |
0.75 |
1.00 |
0 |
1.14 |
|
Copper Salts |
0.75 |
0 |
0 |
1.29 |
|
Spermaceti (Physeter catodon) |
0.75 |
0.87 |
0 |
0 |
|
Honey |
0.70 |
1.94 |
0.09 |
0 |
|
Larch Oil (Larix spp.) |
0.70 |
0.50 |
0 |
0 |
|
*Gum Guaiac (Guaiacum spp.) |
0.69 |
1.06 |
0.54 |
0.16 |
|
Magnesium Sulfate |
0.58 |
0.06 |
0 |
0.49 |
|
†Valerian (Valeriana officinalis) |
0.53 |
3.81 |
0.18 |
0.65 |
|
Potassium Nitrate |
0.50 |
2.56 |
0.36 |
0 |
|
Chamomile (Anthemis nobilis) |
0.49 |
0.25 |
0.54 |
0.16 |
|
Potassium Sulfate |
0.47 |
0.69 |
0.18 |
0.65 |
|
Tobacco (Nicotiana tabacum) |
0.44 |
0 |
0.27 |
0 |
|
Active Ingredient |
Bartlett |
Rowe |
Aspinwall |
Townsend |
|||||||||
|
*Antimony and Antimonial Salts |
0.40 |
2.49 |
1.35 |
6.63 |
|||||||||
|
Sulfuric Acid |
0.38 |
1.62 |
0.18 |
0.16 |
|||||||||
|
*Sulfur |
0.37 |
0.69 |
0.09 |
0 |
|||||||||
|
Alcohol |
0.32 |
0.56 |
0 |
0.48 |
|||||||||
|
Zinc Salts |
0.31 |
0.56 |
0.63 |
1.29 |
|||||||||
|
*Cinnamon (Cinnamonum zeylanicum et al.) |
0.31 |
0.06 |
0 |
0.32 |
|||||||||
|
*Gum manna (Fraxinus ornus) |
0.30 |
0.75 |
0 |
0 |
|||||||||
|
*Squills (Urginea maritima) |
0.29 |
1.06 |
0.72 |
1.94 |
|||||||||
|
*Capivi (Copaifera officinalis) |
0.29 |
1.19 |
0 |
0 |
|||||||||
|
Magnesium Carbonate |
0.29 |
0.81 |
0.09 |
0 |
|||||||||
|
Marsh Mallow (Althea officinalis) |
0.29 |
0 |
0 |
0 |
|||||||||
|
Ammonium & Ferric Chorides, mixed |
0.27 |
0 |
0 |
1.13 |
|||||||||
|
†Black Hellebore (Helleborus niger) |
0.26 |
0 |
0 |
0 |
|||||||||
|
Potassium Citrate |
0.21 |
0 |
0 |
0.65 |
|||||||||
|
Ox hooves (Bos spp.) |
0.21 |
0.31 |
0 |
0 |
|||||||||
|
Benzoic Acid (extracted from Styrax spp.) |
0.15 |
0.75 |
0 |
0.32 |
|||||||||
|
*Contrayerva (Dorstenia contrayerva) |
0.15 |
0.37 |
0.54 |
0 |
|||||||||
|
*Dragon’s Blood, Dragon Tree (Dracena draco) |
0.14 |
0 |
0 |
0 |
|||||||||
|
*Gum Arabic (Acacia spp.) |
0.12 |
0.31 |
0.09 |
0 |
|||||||||
|
*Gentian (Gentiana spp.) |
0.11 |
0 |
0 |
0 |
|||||||||
|
Sassafras (Sassafras albidum) |
0.11 |
0 |
0 |
0 |
|||||||||
|
Potassium Carbonate |
0.11 |
0.69 |
0.45 |
0 |
|||||||||
|
*Orange Peel (Citrus aurantium) |
0.09 |
0 |
0.09 |
0 |
|||||||||
|
Ichthyocolla, Fish Glue (Acipenseridae) |
0.09 |
0 |
0 |
0 |
|||||||||
|
†Juniper (Juniperus spp.) |
0.09 |
0.25 |
0 |
0 |
|||||||||
|
Curcuma, Turmeric (Curcuma longa) |
0.06 |
0.37 |
0.18 |
0 |
|||||||||
|
Sodium Sulfate |
0.06 |
1.94 |
0.18 |
0.16 |
|||||||||
|
Balsam Fir (Abies balsamea) |
0.05 |
0.12 |
0 |
0 |
|||||||||
|
Calcium Salts |
0.05 |
1.50 |
0.09 |
0.65 |
|||||||||
|
Peppermint (Mentha piperita) |
0.05 |
0.06 |
0.09 |
0.16 |
|||||||||
|
*Balsam of Peru (Myroxylon pereirae) |
0.03 |
0.37 |
0 |
0.32 |
|||||||||
|
Galingale (Cyperus spp.) |
0.03 |
0 |
0 |
0 |
|||||||||
|
*Gum Ammoniac (Dorema ammoniacum) |
0.03 |
1.44 |
0 |
0 |
|||||||||
|
*Ipecac (Cephaelis ipecacuanha) |
0.03 |
0.44 |
0.54 |
1.14 |
|||||||||
|
Pink Root (Spigelia marilandica) |
0.03 |
0.12 |
0.09 |
0 |
|||||||||
|
Potassium Aluminum Sulfate |
0.03 |
0 |
0 |
0 |
|||||||||
|
Sodium Carbonate |
0.03 |
0 |
0.09 |
0 |
|||||||||
|
*Betel Palm (Areca catechu) |
0.02 |
0 |
0 |
0 |
|||||||||
|
Ivy (Hedera helix) |
0.02 |
0 |
0 |
0 |
|||||||||
|
*Nutmeg & Mace (Myristica fragrans) |
0.02 |
0 |
0 |
0.16 |
|||||||||
|
Elderberry (Sambucus canadensis) |
0.02 |
0 |
0 |
0 |
|||||||||
|
Ammonium Acetate |
0.02 |
0 |
24.91 |
0.16 |
|||||||||
|
Barium Chloride |
0.02 |
0 |
0 |
0 |
|||||||||
|
Sodium Chloride |
0.02 |
0 |
1.34 |
0.32 |
|||||||||
|
Silver Nitrate |
0 |
0.31 |
0 |
0 |
|||||||||
|
Active Ingredient |
Bartlett |
Rowe |
Aspinwall |
Townsend |
|||||||||
|
Prickly Ash (Zanthoxylum americanum) |
0 |
0.19 |
0 |
0 |
|||||||||
|
*Cascarilla (Croton eleutheria) |
0 |
0.12 |
4.84 |
0.49 |
|||||||||
|
Buckthorn (Rhamnus catharticus) |
0 |
0.06 |
0 |
0 |
|||||||||
|
Bearberry (Arctostaphylos uva-ursi) |
0 |
0.06 |
0 |
0 |
|||||||||
|
Wormsced (Chenopodium ambrosioides var. anthelminticum) |
0 |
0.06 |
0 |
0 |
|||||||||
|
Cerralina (?Quercus cerris?) |
0 |
0.06 |
0 |
0 |
|||||||||
|
Chart (?Powdered Charcoal?) |
0 |
0.06 |
0 |
0 |
|||||||||
|
Ammonium Bicarbonate and Carbamate |
0 |
0.06 |
0 |
1.46 |
|||||||||
|
Tormentilla (Potentilla erecta) |
0 |
0 |
0.09 |
0 |
|||||||||
|
*Scammony (Convolvulus scammonia) |
0 |
0 |
0.09 |
0 |
|||||||||
|
Lettuce (Lactuca sativa) |
0 |
0 |
0.09 |
0.16 |
|||||||||
|
*Bole [?Armeniac] |
0 |
0 |
0.09 |
0 |
|||||||||
|
*Colomba (Swertia caroliniensis) |
0 |
0 |
0 |
0.65 |
|||||||||
|
Barley (Hordeum distichon) |
0 |
0 |
0 |
0.32 |
|||||||||
|
*Quassia (Quassia amara) |
0 |
0 |
0 |
0.32 |
|||||||||
|
Cuckoopint (Arum maculatum) |
0 |
0 |
0 |
0.16 |
|||||||||
|
Bryonia (Bryonia cretica, subsp. dioica) |
0 |
0 |
0 |
0.16 |
|||||||||
Sources: Same as for Table XI.
* Imported, according to Thacher.
† Probably imported.
Table XI lists all the drugs prescribed or, in most instances, dispensed by Drs. Bartlett, Rowe, Aspinwall, and Townsend. The 225 drugs of known composition or therapeutic aim listed included one hundred different ingredients that Thacher considered to be their active components, as listed in Table XII. Some of the drugs listed in Table XI contained two, and a few even three, “active” ingredients (see Appendix I) and some were recognized to contain no substances that had any specific therapeutic effect, only local palliative actions. In Table XI the drugs are assigned to the first of the drug classes listed for each in Thacher’s compendium of current drug usage (see Appendix I for Thacher’s classification), and the classes are given in descending order of Josiah Bartlett’s usage of them.
When the frequencies with which each of the four physicians used the drug classes are ranked, it is clear that the four physicians used the drug classes in similar relative orders of frequency among their patients.18 Although Dr. Thacher provided no data pertaining to the frequency of use of the several classes, the data in Table XI permit us to infer that his Dispensatory does, in fact, reflect a generalized picture of pharmacological indications for drug usage in colonial and federalist New England.
Close inspection of variations in the usage of individual drugs by the four physicians shows that each had a favorite drug for a given situation, such as Bartlett’s remarkable dependence on Elixir of Camphor among the Narcotics, or Aspinwall’s even more remarkable dependence on Spirits of Mindererus as a laxative among the Cathartics. But even discordances such as these do not substantially alter the relative rankings of drug class usage by the two doctors.
In general, Thacher’s classification and, apparently, the four physicians’ patterns of drug use were well grounded on concepts of humoral medicine. That is, the drugs were exploited in attempts to restore imbalances of the humors, by different routes or by different mechanisms of action. Most of the drugs used seem to have been considered as possessing “positive” qualities; most of them were “stimulants” to various portions of weakened or “debilitated” bodies.
Of the drugs listed, the Cathartics are the most prominent in terms of both sheer number and frequency of use. This drug class occupies only a minor role among prescription medicines today. Unfortunately, we do not know just what cathartic agents were used to compound a substantial proportion of many of the preparations given by any of the four physicians. Nevertheless, their supposed pharmacological function is clear. A few of the agents listed were obviously not used only because they promoted evacuations from the bowel, drugs such as Van Swieten’s Antivenereal and Essence Veneris, but it is difficult to believe that there were many patients with syphilis or gonorrhea in the two rural practices where those drugs were used.
Bartlett did not rely on Elixir of Camphor, the Narcotic that he used most often, for its analgesic properties, but for its putative sedative effect. The opiate analgesics were used with approximately equal frequencies by all four physicians. Thacher’s definition of Narcotics (see Appendix) included the use of opiates for their constipating, or antidiarrheal, property. The specific opiates used confirm my earlier hypothesis that more potent forms of the same agent tend to supplant less potent ones, the reverse of Gresham’s Law. In these four practices, Paregoric (and its equipotent analog Elixir Asthmaticus) were used much more frequently than the older, less potent, opiates such as Diacodium and Theriac, which Thacher recognized were unreliable.19
71. Ledger of Dr. Benjamin Rowe, Jr., of East Kensington, New Hampshire. These two pages illustrate one common form of colonial medical accounts, on a day-by-day basis. Courtesy Boston Medical Library.
72. Ledger of Dr. William Aspinwall of Brookline, near Boston. These two pages illustrate another common form of colonial medical accounts, organized by heads of households. Courtesy Boston Medical Library.

73. Dr. Josiah Bartlett (1729–1795). Pencil sketch by John Trumbull, 1790. Courtesy New Hampshire Historical Society, Concord.

74. Surgical needles of Dr. Josiah Bartlett. Photograph by Bill Finney. Courtesy New Hampshire Historical Society, Concord.
75. Portable scales and weights of Dr. Josiah Bartlett. Photograph by Bill Finney. Courtesy New Hampshire Historical Society, Concord.
76. Drug chest of Dr. Josiah Bartlett. Photograph by Bill Finney. Courtesy New Hampshire Historical Society, Concord.
The two country doctors prescribed Tonic drugs more frequently than their urban colleagues. Of these drugs, the Virginia Snakeroot (Radix Serpentina) was the most commonly administered by all four physicians. Bartlett was the only one to rely heavily on the patented Stoughton’s Elixir. It seems likely that the Tonics may be the most “typically New England” of all these ancient drug classes. They rank second in mere numbers of drugs assigned to each class, and third in frequency of use. More important, the word “tonic” remains in common use—in New England, at least—today. The most successful nineteenth-century patent medicines were those advertised as having tonic properties, which carried implicit promises of benefits that would be desirable to the expanding American population. Perhaps it is not too cynical to suggest that Americans, uniquely among national groups, find special merit in agents that are supposed to provide additional tone—extra strength—to the spirit as well as to the body.
Cortex Peruviana was used, for its Astringent properties, more often than any other active principle (except for Camphor in Josiah Bartlett’s practice). The Peruvian Bark was also used in more different preparations than any other agent except, perhaps, opium. Only Aspinwall seems to have preferred another Astringent, Cascarilla, probably as a substitute for the Bark.
Because the Astringent Calybeate was virtually always prescribed for young girls with chlorosis, (a form of iron-deficiency anemia characterized by greenish skin color), the data in Table XI permit the inference that iron deficiency was more common in the country practices than in the city. In general, the four physicians used similar amounts of Astringents throughout their practices.
The country doctors were more likely to prescribe Antispasmodics than their Boston colleagues. Among these drugs Bartlett preferred Volatile Drops, probably an extract from the Cajeput tree, while Rowe preferred Valerian Root. The Boston physicians seldom used any Antispasmodic, and they used Epispastics less frequently than Bartlett and Rowe. Although Aspinwall used Emetics only sparingly, his colleagues used them often, especially Townsend. If the “Emetic” often administered by all but Aspinwall is the “Emetic Weed” (Lobelia inflata) described by Thacher, it is one of the few native plants that found major use in early American medicine. Aspinwall used so many available drugs so seldom, and Spirits of Mindererus so often, that one is tempted to think that he employed that remedy as a sort of panacea, that he thought it to be effective in a wide spectrum of disease.
We have already seen that dropsy, even in the eighteenth century recognized as the chief indication for Diuretic therapy, was diagnosed in about two to five percent of New Hampshire and Boston deaths. The frequency with which the four physicians prescribed Diuretics is entirely consistent with the mortality data in Table VIII. Of these drugs, Squill was regarded as the drug of choice, although Bartlett preferred Ol Terebinth. (Digitalis had been introduced to America through New Hampshire in 1787, but, because the leadership of the Massachusetts Medical Society remained unconvinced of the new wonder drug’s virtues, it would not gain general acceptance until after the turn of the century; consequently, digitalis does not appear in any of the ledgers studied.20)
We are not particularly surprised at the infrequent use made of the remaining classes of internal medications described by Thacher. Worms, uterine diseases, stones, and probably gastric hyperacidity (however it was diagnosed) were not common diseases. And the infrequent use of drugs such as Escharotics, Sialagogues, Expectorants, Errhines, and Diluents suggests that those classes had for some time been recognized as not very useful.
Dr. Townsend, in Boston, used external medications more often than the other three practitioners, of whom Aspinwall used them the least often. Some of these drug preparations may have been administered for the treatment of internal diseases, not only skin conditions. Therefore, it is difficult to ascertain patterns of use among the Emollients and Plasters.
Over the long period of Josiah Bartlett’s practice only one new drug appears for the first time after the first quarter of ledger pages. He first used Sal Nitre in the second quarter (1758–1764) and was using that Refrigerant in 1.6% of his patients by the end of his career. Over the four quarters of Bartlett’s ledger pages, the only drugs whose usage steadily increased were Castor Oil (1.4% to 4.7%), Radix Serpentina (0.6% to about 3.5%), Cremor Tartar (0.6% to 1.4%), Spermaceti (0.1% to 1.2%), and Opiates (2.3% to 5.0%). During the same thirty-seven years, Bartlett’s use of Cantharides and other Epispastics fell (2.0% to 0.5%) as did his use of Lavender (3.5% to 0.5%). He used the Alexipharmical Tincture increasingly often over the first three quarters (2.3% to 7.5%), but in the last quarter he used it relatively rarely (0.6%). And he provided his patients with Directions for self-care increasingly often over the entire period (0.9% to 6.4%). He used all the other drugs at similar frequencies throughout his entire practice. However, at least for Sal Nitre, Castor Oil, Radix Serpentina, Cremor Tartar, Spermaceti, and Opiates, there is some evidence that Dr. Bartlett became increasingly persuaded, perhaps through firsthand observation and experience, of their clinical efficacy. Similarly, he must have found little evidence that either Cantharides or Lavender should be used as often as he had been using them. And he must have begun to realize, after the first few years of his practice, that his patients were able to provide some of their own care, without the necessity (and, presumably, the expense) of further professional visits. Thus, Bartlett seems to have been satisfied with the therapeutic results of most of the drugs he used, for whatever reasons, because he continued to use virtually all of them in similar proportions for almost forty years, and introduced no major new therapies into his regular practice.
The frequencies with which the four practitioners prescribed the drug components that Thacher presumed to be the drugs’ pharmacologically active ingredients are arranged in the order with which Bartlett prescribed them in Table XII.21
Drs. Bartlett and Rowe were the most alike in their uses of these agents.22 Although Bartlett’s drug use was also proportional to those of Drs. Aspinwall and Townsend in Boston, the two rural New Hampshire physicians were more alike in their uses of drugs than they were like their Boston colleagues, as measured by the absolute values of the correlation coefficients.23 The two Boston physicians did not use the drugs they used for similar relative frequencies of their patients.24 Because Dr. Aspinwall used both Aloes and Ammonium Acetate (as Spirits of Mindererus, originally extracted from Aloes), in extraordinarily high proportions of his patients (25.45% and 24.91%, respectively), the physicians’ uses of drugs were compared after omitting those two drugs. When their prescriptions for Aloes and Ammonium Acetate are not taken into account, Dr. Aspinwall’s drug use is highly correlated with those of Dr. Bartlett and Dr. Townsend,25 although Dr. Townsend still seems to have differed somewhat in his use of pharmacologically active agents as the four physicians understood them.
The data in Table XII show that they differed more in their uses of the drugs that any of them used the most often than in their uses of drugs that any of them used least often (in fewer than about 1.0% of patients). Thus, we can infer that drugs which seldom found use in medical practice were used about equally infrequently by all the physicians studied, but that they differed most in their “favorite” drugs, those that they felt were most beneficial to the most patients, even for the same disease state, as seen in Table XI. We can only, hope that discovery of more detailed physicians notes, including information pertaining to both diagnosis and treatment, will someday permit us to understand better how physicians chose drug therapies for patients with demonstrably similar or identical illnesses.
Of the one hundred ingredients listed in Table XII, sixty-eight percent were of botanical origin, twenty-six percent were of chemical or mineral origin (including a few that could be made in eighteenth-century laboratories although originally they had been extracted from plants), and six percent were animal products (including two from insects).
Distributions of patients, drugs, and active ingredients of drugs among practices of four colonial New England physicians.
| Bartleet | Rowe | Aspinwall | Townsend | |
|---|---|---|---|---|
|
% of all 7095 patients in ledgers sampled treated by: |
52 |
16 |
21 |
11 |
|
% of all 225 drugs listed in Table XI administered by: |
72 |
51 |
42 |
40 |
|
% of all 225 drugs listed in Table XI administered only by: |
21 |
7 |
4 |
9 |
|
% of all 100 ingredients listed in Table XII administered only by: |
12 |
7 |
2 |
5 |
Sources: Tables I, XI, and XII.
table xiv
Occurrence of drugs and active ingredients of drugs among four colonial New England medical practices.
| One practice only | Two practices | Three practices | Four practices | |
|---|---|---|---|---|
|
% of all 225 drugs listed in Table XI used in: |
41 |
26 |
19 |
14 |
|
% of all 100 active ingredients listed in Table XII used in: |
27 |
20 |
21 |
32 |
Sources: Tables I, XI, and XII.
As shown in Table XIII, Bartlett administered a larger number of different drugs in his practice than did his three colleagues, and he used more drugs that were not used by the other three than did any of them. Because more than half of all the patient visits represented in the total sampling were Bartlett’s, and because his practice spanned the longest time, the greater diversity among the drugs he employed is not surprising.
Table XIV shows that only fourteen percent of all the drugs, but about a third of their putative active ingredients, were administered by all four of the physicians studied. Only about one-fourth of all these ingredients were employed by only one of the four physicians, and these chiefly among the least frequently used preparations (see Table XII). These data are consistent with the multiplicity of the most commonly used drugs made from the same raw materials, and with the evidence that each physician tended to rely on different preparations within major drug classes. As is clear in Table XII, those active ingredients that were used the most often by any one of the four physicians were used by all the other three as well.
Sources of Drugs
The microfilm edition of Josiah Bartlett’s papers also includes forty-three receipts or orders for drugs that he obtained from eight “wholesalers” in northeastern Massachusetts and southeastern New Hampshire from 1750 to 1772. The forty-three orders comprise eighty-nine different drugs or drug ingredients ordered a total of 502 times. Only three items he ordered do not appear among the drugs Bartlett prescribed or dispensed for his patients.
In order to assess the extent to which the drugs Bartlett ordered reflect his usage of them, correlation coefficients were computed. For all eighty-nine different drugs he ordered, the correlation between the frequencies of his orders and his prescriptions for the same drugs was low but significant.26 When Elixir of Camphor is omitted from the correlation computation (because it appears only twice among 502 drug items ordered, although Bartlett prescribed it for over twelve percent of his patients), the degree of correlation between drug orders and drug prescriptions increases markedly.27 And, for five other drugs there were marked (five to 76-fold) discordances between orders and prescriptions; when they are omitted, the correlation increases still further.28 These data lead to the inference that although the drug orders do indeed reflect Bartlett’s prescribing patterns, the orders do not provide a complete picture of the drugs he used in providing therapy for his patients. Most of the discordance is, of course, attributable to the incompleteness of the drug orders that have survived. Nevertheless, in the absence of a proven complete set of orders, they cannot be considered to reflect a physician’s everyday practice to the same extent that his ledgers can.
Towards the end of the century Jeremy Belknap solicited from physicians throughout New Hampshire their opinions about the medically useful indigenous plants of the state. His final list was (the Latin names in parentheses are Belknap’s, and the asterisks indicate names that also appear among the active ingredients listed in Table XII):
- * Sassafras (Laurus sassafras)
- Spice-wood, or Fever-bush (Laurus benzoin*)
- Oil-nut, or Butter-nut (Juglans cathartica)
- *Pitch pine (Pinus taeda), for Ol Terebinth
- *Larch (Pinus larix), for Ol Terebinth
- *Fir (Pinus balsamea)
- *Hemlock (Pinus abies)
- *Juniper (Juniperus sabina), an Anthelminthic
- White willow (Salix alba), a Cortex Peruviana* substitute
- Black poplar (—), like Balsam of Peru*
- Ginseng (Panax trifolium)
- *Prickly ash (—), for chronic rheumatism
- *Black elder (Sambucus niger)
- Red elder (Viburnum opulus)
- Maiden-hair (Adianthus pedatuus)
- Sarsaparilla (Aralia)
- Snakeroot (Polygala senega)
- Poke, Indian tobacco (—), with strong Narcotic quality
- Witch hazel (Hamamelis), for inflammation
- *Lobelia [L. inflata], a strong Emetic
- Lobelia cardinalis, “employed in the cure of a disease, with the name of which I will not stain my page” [i.e., syphilis]
- Buckbean (Menyanthes), of “singular use in medicine”
- Skunk cabbage (Arum), for asthmatic complaints
Poisons, also used in the cure of spasmodic diseases:
- Hemlock (Cicuta)
- Thornapple (Datura stramonium)
- Henbane (Hyoscyamus niger)
- Nightshade (Solanum nigrum)
Other poisons, without stated medical uses:
- *Ivy (Hedera helex [sic])
- Creeping ivy, or Mercury (Rhus radicans)
- Swamp sumach (Rhus toxico dendrum)
- Water elder (Viburnum opulus) (same as Red elder above)
- Herb Christopher (Actea spicata)
- Stinking snakeweed (Cliffortia trifoliata)
- White hellebore (Veratrum album)29
Comparing this list of medically useful plants indigenous to New Hampshire with the drugs and active ingredients listed in Tables XI and XII shows that, with the possible exception of Lobelia inflata, if that species was the “Emetic” listed so often by Drs. Bartlett, Rowe, and Townsend, the native vegetable productions of New Hampshire, and perhaps all New England, were insufficient to furnish most of the medical profession’s therapeutic needs.
Of the one hundred active drug ingredients included in Table XII, forty were imported. These forty (marked with an asterisk in the table) constitute fifty-five percent of all the drugs administered by Bartlett and Rowe, forty-one percent of those given by Townsend, and thirty-two percent of those given by Aspinwall. Of the other sixty drug ingredients, about half are inorganic chemicals that were easily prepared by physicians or their drug suppliers. Most of the other half were native plants, but they constitute only a small proportion of all the drugs administered. In general, New England physicians had to rely on imported materials for the drugs they most often prescribed. It would seem, then, that native American plants had not contributed substantially to the list of effective medicines available to colonial New England physicians, and that they were still dependent on drugs procured in other countries long after the Revolution.
Of all the drugs prescribed by the four physicians, 19.4% were inorganic chemicals or purified organic extracts. They constituted only fifteen percent of Bartlett’s practice, but from twenty-four percent, of Rowe’s, to thirty-two percent, of Aspinwall’s (because of his reliance on Ammonium Acetate). These proportions suggest that drugs in the Paracelsian tradition were more important among the urban practices than in rural areas, but that colonial physicians gave Galenic botanical preparations to the majority of their patients.
discussion
Random samplings of data from four physicians’ ledgers support the hypothesis that we can reconstruct the collective routine everyday medical practice of colonial New England doctors from such documents. In addition, this method permits detection of differences among practices in varied settings or among individual practitioners. We do not know the precise indications that led any one of the four physicians to prescribe what he did for any individual patient, or for all patients with the same disease. However, we can still assess the epidemiological data pertaining to the practitioners’ drug use with the help of a standard compendium of eighteenth-century American drug remedies. This use of Thacher’s Dispensatory for interpreting the drug classes the physicians prescribed, or thought would be effective, is warranted because therapy at that time was, as Shryock has pointed out, directed against “general body conditions,” as is implicit in Thacher’s classification.30
The data do not shed much new light on just why physicians chose the drugs they did. Bridenbaugh has observed that “the colonial approach to the healing art came nearer to being ‘scientific’ than most contemporary analyses in Europe.”31 He was referring specifically to published medical papers, especially their empiric qualities, but even the analytical modes of distinguished physicians, as expressed in their papers, must find some reflection in the everyday practices of their colleagues who did not publish.
It is difficult to ascertain the extent to which Bartlett, Rowe, Aspinwall, and Townsend practiced “scientific” medicine. The scientific quality of modern clinical medicine is debated even today.32 Our four practitioners focused their attentions chiefly on morbid states of the humors as the ultimate causes of their patients’ illnesses. If some aspect of one or more humors was present in excess, the patient was treated by measures designed to remove the excess, with drugs like Cathartics or Diaphoretics. If, on the other hand, something was deficient in the humors, restorative measures, like Narcotics or Tonics, were applied. Although strict humoralism was being replaced, in the late eighteenth century, by concepts of excessive or diminished nervous or vascular tension (“solidism”), the therapeutic principles of their treatment, by restoring balance or tension, were similar.33
William Heberden’s chapter “Ratio Medendi” sets forth a simplified pharmacological rule for determining the choice of an effective agent:
One of the first considerations in the cure of a disease is, whether it require any evacuations; that is, whether it have been the general opinion of practical authors, that emetics, cathartics, diuretics, bleeding, . . . sudorifics, blisters, issues, [errhines], or salivation, have in similar cases been found to be beneficial.
2ndly. Whether it be a distemper, for which any specific, or certain remedy, has been found out. . . . [T]he honour of this title may be justly claimed by the Peruvian bark for the cure of agues; quicksilver for Venereal disorders; sulphur for the itch; and perhaps opium for some spasms; and Bath waters for the injury done to the stomach by drinking ... Borax has been celebrated . . . for aphthae; the Portland powder for the gout; squills and the fetid gum-resins for the asthma; soap-ley for the gravel and stone; hemlock for cancers; . . . antimony for continual fevers; sugars of lead for haemorrhages; and some few others for other distempers.
Though, among the pretended specifics, some have very little virtue, and others may be inconstant in their operations; yet, if a physician be satisfied that they are safe, there may be many occasions when he may with propriety employ them.
3dly. Vomiting, purging, pain, and other troublesome symptoms, are in many cases so urgent, as to make some present relief indispensably requisite; for the procuring of which, opium is very commonly the most effectual means.
4thly. In long and obstinate diseases, in which no particular remedy is found to have succeeded, it is often advisable to have recourse to the general means of strongly affecting, and of making considerable changes in the state of the body; in hopes, by this shock, of dislodging the cause of the disease. For this end, mercury, antimony, hemlock, and electrification, are sometimes employed.
Lastly, where there is no room for any thing else, there it is the duty of a physician to exert himself as much as possible in supporting the powers of life, by strengthening the appetite and digestion, and by providing that the stools, and sleep, and every other article of health, shall approach as nearly as may be to its natural state.34
Eighteenth-century physicians are often accused of being empiric in their therapeutics. Perhaps it is unfair to use the word “empiric” in a pejorative sense. One English physician in 1787 described empiricism as being “derived from a Greek word which signifies experience, the foundation of all science, especially of physick.” Levi Bartlett points out with pride that his father was not a rationalist who depended only on theory:
Dr. B. was a great observer of nature in all Disseases, and never was bound to dogmatical Medical rules in prescribing for his Patients. Having emancipated his Mind from the tramels of Theological and Medical rules didactically imposed by art, he laid the foundation of bottoming all correct knowledge upon the course of Nature leading to usefulness, readily perceiving the love of Deity to all his works in giving to Mind a beneficent pleasure of Goodness directed by Reason & Conscience, and to the Body the Vis Medicatrix natura[e] instead of traditionary rules. . . . Dr. Bartlett began his carreer of public usefulness by accurately discriminating between truth and error. By this discriminating power he became a popular Physician, had a large run of practice which was both lucrative & honorable to himself & highly useful to the people.
The proud son later gives one example of how his father, after making a series of clinical observations, proved to his own satisfaction that the Angina tonsillaris maligna was not the sort of disease that medical tradition had always specified, and so changed his therapeutic approach to it.35
The title page of the bills of mortality for Benjamin Rowe, Jr.’s Kensington contains a poem by Henry Mellen of nearby Dover that illustrates one literate layman’s concept of the relationship between science and clinical medicine:
How oft grim Death withdraws his venom’d dart,
Sooth’d by the influence of the healing art?
When Science, skill and caution guide the hand
Diseases fly, and pain obeys command;
While from the hand of ignorance ensue
A thousand ills, that nature never knew.36
Today’s science implies observation, identification, description, experimental investigation, and theoretical explanation of natural phenomena. The epithet “empiric” was not always derogatory in the late eighteenth century. Heberden’s “Ratio Medendi” includes elements of both rationalism, insofar as pathophysiological concepts are concerned, and empiricism, in regard to assessing drug efficacy and safety. It would seem that our four physicians practiced during the period when total dependence on theory was being replaced by tentative verification by experimentation, a process that could not come into full flower until the mid-nineteenth century. They appear, from even the indirect evidence available to us, to have practiced a rudimentary form of what we can now recognize as science. In the absence of new concepts of physiological function, concepts which would eventually displace both humoral theory and concepts of vascular or nervous disfunction, they could not make many significant changes in their therapeutic methods. It is chiefly the lack of what we can now recognize as explicitly designed negative or positive controls that prevents the therapeutics of our four colonial New England physicians from being completely “scientific” in the modern sense.37 The overall concordance in the proportions of their prescriptions which can be assigned, however tentatively, to a standard drug classification suggests that Drs. Bartlett, Rowe, Aspinwall, and Townsend worked from a common understanding of drug actions and with similar patient populations. The latter conclusion can also be verified from the bills of mortality for the physicians’ respective communities. The similarities among their practices suggest that the four were inheritors, and exploiters, of a common medical “science,” however that is defined.38
The differences among the four practices probably do not tell us as much about differences among their patient populations as about differences in their methods of choosing drugs for their patients. Bartlett introduced only one new drug into his practice during almost four decades, and altered his use of only a very few others; we have no corresponding evidence for the other three physicians. Shryock has suggested that, in the seventeenth and eighteenth centuries, “Remedies seem to have accumulated on a trial-and-error basis.”39 We have little evidence for such trials, or errors, from the four sets of ledgers, or that any of the four physicians discarded any drugs outright. The larger number of drugs used only by Bartlett than those used only by any of the others does not refute this. It is likely that larger samplings of the other three physicians’ ledgers would have revealed that they did, in fact, use other kinds of drugs. In any event, the majority of the drugs used by only one or two of the four were used seldom or rarely even by them.
It seems highly unlikely that any of the four physicians would have used, or would have continued to use, any drugs that he did not observe to be both effective and safe for his patients. Of the two, safety would seem most likely to have been sacrificed if efficacy could be demonstrated. Perhaps it is, then, reasonable to conclude that colonial New England physicians depended first on the scientific inquiries of others, and on their own empiric observations, in choosing a drug for any patient, and then on their own clinical observations for making any alterations in their therapeutic plans. It is not difficult to understand this kind of thought process as meeting criteria for “science” that were prevalent in the late eighteenth century, or in the late twentieth century.
It is not possible to assess the extent to which colonial American physicians actually affected the health of their patients. The majority of the drugs they used have little, if any, proven therapeutic value when measured by today’s yardsticks of efficacy. Yet these physicians can hardly be accused of quackery, charlatanism, or other nonprofessional goals. It seems that two factors contributed most to the health and health care of colonial Americans.
First, their physicians could not recognize that the remedies they prescribed for their patients were not effective by modern criteria, nor could their patients. Consequently, the remedies that were then employed can, perhaps, be considered as having been beneficial in ways different from those demanded by modern concepts of pharmacological effectiveness. It is possible that the mere provision of some kind of professional attention, regardless of its merits, was in some way beneficial to at least some colonial patients, although a sort of mass placebo effect probably need not be postulated as an explanation. Physicians tried their best to do what they could for their patients; it was not the doctors’ fault that their drug remedies are now known not to be very helpful.
A more concrete clue to the apparent efficacy of colonial remedies comes from the records of the Philadelphia Dispensary. Table XV lists the diagnoses made by Dispensary physicians from late 1786 through 1792, and their clinical outcomes.40 Because these are the most extensive data of this kind for any place in eighteenth-century America, they are given here in full. Even on cursory inspection, these data suggest that the vast majority of patients recovered, or could be cured surgically, and that death was an infrequent outcome of disease in adults.
Although some of the Philadelphia diagnoses were not made in New England, and vice versa, as seen by comparing the causes of death listed in Tables VIII and XV, the overall pictures must have been similar in both areas (unless distorted by major epidemics). Infectious diseases were the most common of all, as we’ve already noticed in Table VIII, in terms of both morbidity and mortality, yet they seldom (5.5%) resulted in death (in adults). Noninfectious disorders of the nervous and cardiovascular systems were relatively rare, but they often resulted in death. (Dropsy, or hydrops, is strangely missing from the Philadelphia list. However, because these diagnoses focus on single clinical signs, cases that would have been diagnosed as dropsy in New England may be camouflaged by several cardiovascular diagnoses.)
Diagnoses, cure rates, and death rates among 9683 patients treated at the Philadelphia Dispensary from December 1786 through November 1792. Patients not accounted for in the sums of patients cured and those who died from each disease or disease category were either transferred to other facilities, such as the Pennsylvania Hospital, or otherwise lost to follow-up. The committee that compiled the original tabulation utilized Cullen’s nomenclature as best it could. Their diagnoses have been rearranged alphabetically (to facilitate finding any given diagnosis) according to modern pathophysiological concepts, insofar as possible, although many eighteenth-century diagnoses were not understood in the same ways as in the twentieth century. Only diagnoses which cannot easily be found in modern medical dictionaries are further identified in parentheses in the table; parenthetical definitions that include an equal sign (=) are synonyms used by the authors of the original data.
| % all diagnoses | Cure rate* (%) | Death rate* (%) | % all deaths† | |
|---|---|---|---|---|
| Diagnoses | ||||
|
infectious diseases |
65.14 |
84.0 |
5.5 |
79.21 |
|
Abscessus |
0.38 |
91.9 |
5.4 |
0.46 |
|
Anthrax |
0.02 |
100.0 |
0 |
0 |
|
Aphtha (Thrush) |
0.17 |
87.5 |
6.3 |
0.23 |
|
Caries & Odontalgia |
0.23 |
77.3 |
0 |
0 |
|
Catarrhus |
5.04 |
93.4 |
0.6 |
0.68 |
|
Cholera |
1.06 |
96.1 |
3.9 |
0.91 |
|
2.95 |
86.4 |
12.6 |
8.22 |
||||||||||||||||||||
|
Convulsio |
0.31 |
80.0 |
16.7 |
1.14 |
|||||||||||||||||||
|
Cynanche Maligna |
0.01 |
0 |
100.0 |
0.23 |
|||||||||||||||||||
|
Cynanche Parotidea |
0.18 |
94.4 |
0 |
0 |
|||||||||||||||||||
|
Cynanche Tonsillaris |
0.45 |
97.7 |
2.3 |
0.23 |
|||||||||||||||||||
|
Cynanche Trachealis |
0.25 |
62.5 |
33.3 |
1.83 |
|||||||||||||||||||
|
Diarrhoea |
3.47 |
85.4 |
10.4 |
7.99 |
|||||||||||||||||||
|
Dysenteria |
2.33 |
90.7 |
5.3 |
2.74 |
|||||||||||||||||||
|
Eruptiones |
1.44 |
92.1 |
0.7 |
0.23 |
|||||||||||||||||||
|
Erysipelas |
0.40 |
82.1 |
0 |
0 |
|||||||||||||||||||
|
Febris Quotidiana |
2.33 |
96.5 |
0 |
0 |
|||||||||||||||||||
|
Febris Tertiana |
1.70 |
97.0 |
0 |
0 |
|||||||||||||||||||
|
Febris Quartana |
0.14 |
100.0 |
0 |
0 |
|||||||||||||||||||
|
Febris Hectica [?Phthisic?] |
0.01 |
0 |
100.0 |
0.23 |
|||||||||||||||||||
|
Febris Puerpera |
0.19 |
83.3 |
16.7 |
0.68 |
|||||||||||||||||||
|
Febris Remittens |
1.53 |
88.5 |
5.4 |
1.83 |
|||||||||||||||||||
|
Febris Synocha/Synochus (Continued Fevers) |
0.55 |
96.2 |
1.9 |
0.23 |
|||||||||||||||||||
|
Febris Typhus |
0.96 |
62.4 |
26.9 |
5.71 |
|||||||||||||||||||
|
Febris Verminosa |
0.02 |
100.0 |
0 |
0 |
|||||||||||||||||||
|
Gangrene (=Sphacelus) |
0.07 |
0 |
85.7 |
1.37 |
|||||||||||||||||||
|
Gonorrhoea |
1.71 |
87.3 |
0 |
0 |
|||||||||||||||||||
|
Hepatitis |
0.41 |
80.0 |
12.5 |
1.14 |
|||||||||||||||||||
|
Herpes |
0.93 |
84.4 |
0 |
0 |
|||||||||||||||||||
|
Nephritis |
0.27 |
57.7 |
3.8 |
0.23 |
|||||||||||||||||||
|
Otalgia |
0.06 |
100.0 |
0 |
0 |
|||||||||||||||||||
|
1.41 |
47.1 |
3.6 |
1.08 |
||||||||||||||||||||
|
Amaurosis (Blindness) |
0.02 |
0 |
0 |
0 |
|||||||||||||||||||
|
Cephalgia (Headache) |
0.25 |
95.8 |
0 |
0 |
|||||||||||||||||||
|
Chorea |
0.06 |
0 |
0 |
0 |
|||||||||||||||||||
|
Epilepsia |
0.62 |
20.0 |
0 |
0 |
|||||||||||||||||||
|
Hydrocephalus Acutus |
0.03 |
0 |
100.0 |
0.68 |
|||||||||||||||||||
|
Hydrocephalus Chronicus |
0.02 |
0 |
0 |
0 |
|||||||||||||||||||
|
Hydrocephalus Externus |
0.01 |
0 |
0 |
0 |
|||||||||||||||||||
|
Hydrocephalus Internus |
0.09 |
22.2 |
22.2 |
0.40 |
|||||||||||||||||||
|
Ischias (Sciatica) |
0.03 |
100.0 |
0 |
0 |
|||||||||||||||||||
|
Spasmi |
0.15 |
100.0 |
0 |
0 |
|||||||||||||||||||
|
Surditas (Deafness) |
0.03 |
0 |
0 |
0 |
|||||||||||||||||||
|
Syncope |
0.02 |
100.0 |
0 |
0 |
|||||||||||||||||||
|
Vertigo |
0.08 |
100.0 |
0 |
0 |
|||||||||||||||||||
|
primary cardiovascular disorders |
2.47 |
42.1 |
23.3 |
12.78 |
|||||||||||||||||||
|
Anasarca |
0.70 |
44.1 |
26.5 |
4.11 |
|||||||||||||||||||
|
Apoplexia |
0.06 |
16.7 |
83.3 |
1.14 |
|||||||||||||||||||
|
Ascites |
0.41 |
22.5 |
35.0 |
3.20 |
|||||||||||||||||||
|
Atrophia |
0.19 |
27.8 |
55.6 |
2.28 |
|||||||||||||||||||
|
Dyspnea |
0.04 |
100.0 |
0 |
0 |
|||||||||||||||||||
|
Hemoptoe (Hemoptysis) |
0.32 |
90.3 |
3.2 |
0.23 |
|||||||||||||||||||
|
Hydrothorax |
0.14 |
28.6 |
28.6 |
0.91 |
|||||||||||||||||||
|
Palpitatio |
0.02 |
0 |
0 |
0 |
|||||||||||||||||||
|
Paralysis and Hemiplegia |
0.59 |
35.0 |
7.0 |
0.91 |
|||||||||||||||||||
|
0.01 |
100.0 |
0 |
0 |
||||||||||||||||||||
|
Podagra (Gout) |
0.06 |
16.7 |
16.7 |
0.23 |
|||||||||||||||||||
|
Rachitis (Rickets) |
0.04 |
0 |
50.0 |
0.46 |
|||||||||||||||||||
|
Rheumatismus |
6.05 |
73.0 |
0.5 |
0.68 |
|||||||||||||||||||
|
disorders of the gastrointestinal tract |
8.42 |
89.5 |
1.1 |
2.06 |
|||||||||||||||||||
|
Colica |
2.38 |
96.5 |
2.6 |
1.37 |
|||||||||||||||||||
|
Constipatio & Obstipatio |
0.88 |
98.8 |
0 |
0 |
|||||||||||||||||||
|
Dyspepsia, Gastrodynia, & Pyrosis (Stomachache) |
3.75 |
90.6 |
0 |
0 |
|||||||||||||||||||
|
Dysphagia |
0.04 |
75.0 |
0 |
0 |
|||||||||||||||||||
|
Fistula in Ano/Perinaeo |
0.07 |
14.3 |
14.3 |
0.23 |
|||||||||||||||||||
|
Gastritis |
0.02 |
100.0 |
0 |
0 |
|||||||||||||||||||
|
Haemorrhoids |
0.37 |
91.7 |
0 |
0 |
|||||||||||||||||||
|
Hematemesis |
0.11 |
81.8 |
9.1 |
0.23 |
|||||||||||||||||||
|
Hernia Inguinalis |
0.17 |
31.3 |
0 |
0 |
|||||||||||||||||||
|
Icterus (Jaundice) |
0.28 |
77.8 |
3.7 |
0.23 |
|||||||||||||||||||
|
Melaena |
0.02 |
100.0 |
0 |
0 |
|||||||||||||||||||
|
Physconia (Abdominal Swelling) |
0.12 |
41.7 |
0 |
0 |
|||||||||||||||||||
|
Prolapsus Ani |
0.07 |
85.7 |
0 |
0 |
|||||||||||||||||||
|
Schirms (?Cirrhosis, ?Tumor) |
0.05 |
40.0 |
0 |
0 |
|||||||||||||||||||
|
Tympanites |
0.04 |
50.0 |
0 |
0 |
|||||||||||||||||||
|
Vomitus |
0.05 |
100.0 |
0 |
0 |
|||||||||||||||||||
|
casualties |
5.58 |
91.9 |
0.7 |
0.92 |
|||||||||||||||||||
|
Asphyxia |
0.02 |
100.0 |
0 |
0 |
|||||||||||||||||||
|
Contusio |
2.81 |
93.4 |
0.4 |
0.23 |
|||||||||||||||||||
|
0.05 |
20.0 |
20.0 |
0.23 |
||||||||||||||||||||
|
Polypus |
0.03 |
0 |
0 |
0 |
|||||||||||||||||||
|
Pemphigus |
0.01 |
100.0 |
0 |
0 |
|||||||||||||||||||
|
Raphania (?Radish or Ergot Poisoning) |
0.01 |
100.0 |
0 |
0 |
|||||||||||||||||||
|
Splenitis |
0.01 |
0 |
100.0 |
0.23 |
|||||||||||||||||||
|
all patients |
(100.0) |
81.3 |
4.5 |
(100.0) |
|||||||||||||||||||
Source: Samuel P. Griffits, J. Morris, John R. B. Rodgers, Caspar Wistar, Jun., William Clarkson, and Michael Leib, [“Return of the Diseases of the Patients of the Philadelphia Dispensary,”] Transactions of the College of Physicians of Philadelphia, 1 (1793), 2–42.
* Fraction of patients with each diagnosis who were cured, or who died, of that disorder,
† Among the 438 patients who died at the Dispensary.
It seems, then, that Josiah Bartlett’s recognition of the vis medicatrix naturae is consistent with the experience of the physicians at the Philadelphia Dispensary. It is only today that we can infer that their “cure” rates were probably independent of the drugs they administered, and that the healing power of nature was more effective than colonial drugs.41
The second major factor contributing to the health of American colonists is more geopolitical than medically scientific, namely, the colonists’ wide dispersal throughout the open countryside, where they were less often subject to communicable disease than in their European homelands. Jeremy Belknap, New Hampshire’s first historian, argued that while European authors might be correct in describing the southern states as less healthy than Europe, the facts pertaining to New Hampshire, and probably other New England states, proved that in that area people were healthier and lived longer. He argued, too, that science, as an integral facet of the Enlightenment, demanded accurate observations before conclusions could be made:
If authors profess to write as philosophers they should seek for information from the purest sources, and not content themselves with theorising on subjects, which can be determined only by fact and observation; or with forming general conclusions from partial reports. If they write as politicians, their aim may indeed be answered by stating facts in a delusive light; and by representing America as a grave to Europeans, they may throw discouragement on emigration to this country. . . . But notwithstanding the dreams of European philosophers, or the interested views of European politicians, America can best be described by those who have for a long time resided in it. . . .
In that part of America which it falls to my lot to describe, an ‘uncleared and uncultivated soil,’ is so far from being an object of dread, that there are no people more vigorous and robust than those who labour on new plantations. . . . This is true not only of the natives of the country, but of emigrants from Europe. It has been a general observation that the first planters in new townships live to a great age. It is also true that the air of our forest is remarkably pure. The tall and luxuriant growth which an European might call ‘rank vegetation,’ not only indicates strength and fertility of soil; but conduces to absorb noxious vapours [which are responsible for so much disease in the southern states]. ... A profusion of effluvia from resinous trees impart to the air a balsamic quality which is extremely favourable to health.... To these observations it may be added, that the northwest wind is the grand corrector of every noxious quality which can exist in the air of America; and whilst that wind prevails, it diffuses health and imparts vigour to the human frame.
There are, indeed, some few situations, even in New-Hampshire, where vapour arising from land overflowed with fresh water, produces bilious and nervous diseases, and the inhabitants are subject to an early lassitude and debility; which is often increased by an injudicious use of spirituous liquors for medical purposes [although it is clear from Table XI that physicians did not prescribe alcohol injudiciously]. . . .
From the tables of mortality which I have collected [see Tables VIII and IX] ... it appears that a very large proportion of people live to old age, and that many of them die of no acute disease but by a gradual decay of nature, [unless] some epidemic disorder prevails, which very seldom happens.42
Belknap’s conclusions are consistent with the calculated life expectancies shown in Table IX, which demonstrates that life expectancy was inversely proportional to population density. Surely such a collector of facts, and he collected many of his medical facts from New Hampshire physicians, cannot have been completely unaware, however much he had to draw on intuition and indirect inference to arrive at his conclusions, that the most that could be expected from New England physicians’ best professional efforts was palliative therapy, that they were generally unable to provide definitive cures in the way we expect of our physicians today. Belknap, and the physicians themselves, probably thought that medicine was as “scientific” as it could be, that it was soundly based on rules of observation and inference, but both were probably sufficiently realistic to recognize that other factors were primary determinants of whether patients recovered from their wounds and illnesses.
None of the four New England physicians whose ledgers have been examined published medical texts or articles. We have, then, virtually no evidence other than that from their ledgers as to their medical practices. Throughout all the collected papers of Josiah Bartlett there are very few references to medical matters. (Of course, Bartlett’s papers have been preserved for two centuries not because of his professional career, but because of his role in Revolutionary politics.) His medical concepts, even those that seemed new to his contemporaries, were solidly based on humoral theory, as is evident from one of the few medical incidents described in his son’s reminiscences of the second person to sign the Declaration of Independence:
In Inflamatory disseases the practice was to keep the sick warm, to keep him from the air & any cool liquids, warm teas & warm stimulating medicines were used to promote a diaphoresis. Dr. B. found by this practice fatal inflamations & sudden putridity destroyed the sick. He changed the course, Ventilated the room, kept but few cloths on the sick, allowed them cool drinks, and every thing which their nature craved; by this means he suppressed many & lightened all inflamatory fevers. This practice afterwards became the general mode.43
It would seem that Bartlett’s practice was consistent with that of most eighteenth-century physicians, countering fever with a cooling form of therapy, as rational humoral theory demanded. His anti-inflammatory therapy may have been novel to the nonprofessionals of Kingston, but not to his professional colleagues throughout the colonies.
In 1783 Bartlett wrote to Benjamin Rush to inquire about a Dr. Martin’s remedy for cancers and scirrous and “schrophalous” tumors, because Bartlett’s daughter had a tumor just below her ear. Bartlett also solicited Rush’s opinion because “I have no very good opinion of Nostrums & quack medicine.” Rush replied that Martin’s remedy was useful, but that Bartlett should prepare it himself, using poke-weed, powder of white hellebore, and nightshade berries, all of which could be regarded as “caustics.” Rush also suggested that the Peruvian bark, gentle exercise, and a cold bath would be helpful. Unfortunately, the outcome of this therapy, if Bartlett tried it, is not known.44
The ledgers show that New England physicians shared a common therapeutic theme, although each employed his own variations on that theme. The evidence as to how they came to share a common mode of practice is only circumstantial. The two New Hampshire physicians received their professional training from relatives, as was often the case, while the two Boston doctors first attended Harvard College and then had further training from two of the country’s leading physicians; Aspinwall also had a pupilage away from home. All but Bartlett had experience as military surgeons, and all but Rowe were active in their state medical societies (although Aspinwall joined the Massachusetts society only long after the ledgers, he had been active in local medical and political affairs for some years before). In fact, Josiah Bartlett had been among the founders, and was the first president, of his state’s medical society. That he had long thought a state society would benefit the profession’s collective expertise, to the advantage of its patients, is evident from his son’s memoir:
Dr. B.’s intention was to increase the knowledge in the healing Art as well as to obtain compensation. He therefore, being always friendly to the neighboring Physicians proposed & effected frequent meetings together in Social compact to converse freely upon & discuss questions & cases in their profession. From ten to Twenty joined & met once, twice or oftener in the year in rotation at each others houses. This was kept up untill the beginning of the Revolution.45
Because Kensington is not far from Kingston or the New Hampshire seacoast towns, it is possible that Rowe joined with area physicians meeting informally even after the Revolution. At least, there was one common final pathway for the exchange of information and opinion that was available to him even before the founding of the New Hampshire Medical Society which he did not join. Because in many, although not in all, ways the four New England physicians shared common bodies of professional experience, and shared them with Thacher as well, we are not surprised that their ledgers reveal a clear pattern of medical therapeutics as practiced in colonial New England.
This work was supported by a grant from the Boston University Graduate School, which is here gratefully acknowledged.
APPENDIX I
Synopsis of the Materia Medica, as Outlined by James Thacher in 1810
general stimulants
A. Diffusible, or Transient, General Stimulants
- 1. NARCOTICS: diminish the actions and powers of the system, without causing sensible evacuation; excite functions of both body and mind; increase the force of pulse and muscular activity; eventually cause sleep. Act via stomach and nerves. Uses: debility, intermittent and typhoid fevers, gout, hysteria; as sedatives; to decrease pain, secretions, and discharges.
- 2. ANTISPASMODICS: like Narcotics, decrease pain and inordinate action, but without causing insensibility and are less diffusible. Uses: same as for Narcotics and Tonics; also, for dentition and worms.
B. Permanent General Stimulants
- 3. TONICS: act on living fiber to strengthen the system, via the stomach, by increasing the force of circulation, animal heat, secretions, digestion, and muscular action. Vegetable tonics are more potent than minerals. Uses: debilities, which include most diseases.
- 4. ASTRINGENTS: diminish increased evacuations, by condensing the simple solids of which the vessels are formed, as some Tonics do. Uses: to decrease evacuations such as hemorrhage, menorrhagia, hemoptysis, diarrhea, excessive sweating, diabetes mellitus, and superficial inflammations (all of which may occur in debilities and intermittent fevers).
local stimulants
- 5. EMETICS: excite vomiting, independent of the volume of material introduced into the stomach or of taste; may promote absorption, or be laxative in low doses. Uses: in conditions accompanied by distention of the stomach, hyperacidity, poisoning, intoxication, biliary jaundice, fever, or dropsy.
- 6. CATHARTICS: augment natural peristaltic flow of intestinal contents to excite purging, and of neighboring organs to increase bile flow and gastric emptying. Aperients are least potent, purgatives are most potent. Uses: constipation, colic, dysentery, fevers, dyspepsia, hypochondriasis, amenorrhea, jaundice, dropsy, apoplexy, coma, mania, headache, rheumatism (as antiphlogistic therapy).
- 7. EMMENAGOGUES: promote menstrual discharge by stimulating uterine vessels. Uses: in decreased menstrual flow.
- 8. DIURETICS: promote urinary discharge by stimulating the secreting vessels of the kidney, or by promoting absorption of fluid by vessels throughout the body. Uses: dropsy; also, calculi, gonorrhea, excessive sweating.
- 9. DIAPHORETICS: increase natural exhalation by the skin, by stimulating the cutaneous exhalant vessels. Sudorifics are more potent than diaphoretics. Uses: dropsy, asthma, dyspepsia, chronic diarrhea, rheumatism.
- 10. EXPECTORANTS: facilitate rejection of mucus and other fluids from lungs and trachea, by an unknown mechanism. Uses: pneumonia, catarrh, asthma.
- 11. SIALOGOGUES: increase salivary discharge by an unknown mechanism. Uses: none apparent.
- 12. ERRHINES: increase mucus or serous discharge from nostrils, or sneezing, because of bitter qualities when applied locally. Uses: headache, earache, ophthalmia, rheumatic affections of the head.
- 13. EPISPASTICS: produce serous or purulent discharge by exciting a previous state of inflammation, when applied topically. RUBEFACIENTS are similar, but do not produce fluid discharge. Uses: pneumonia, gastritis, hepatitis, phrenitis, angina, rheumatism, colic: in toothache, because exciting one pain often relieves another.
agents acting chemically
- 14. REFRIGERANTS: decrease force of circulation and body heat, without decreasing sensibility or nervous energy. Uses: inflammations, fevers of typhoid kind.
- 15. ANTACIDS: neutralize stomach acids. Uses: dyspepsia, diarrhea.
- 16. LITHONTRIPTICS: dissolve uric (“lithic”) acid. Uses: urinary calculi.
- 17. ESCHAROTICS: dissolve animal matter. Uses: skin excrescences, ulcers.
agents acting mechanically
- 18. ANTIHELMINTHICS: expel worms from the intestinal canal, because of the roughness of the drug’s particles, or the drug’s cathartic action.
- 19. DEMULCENTS: prevent the action of acrid and stimulant materials by covering the surface exposed to them with a mild viscid matter. Uses: catarrh, diarrhea, dysentery, calculi, gonorrhea.
- 20. DILUENTS: increase the proportion of fluid in the blood. Synergistic with diuretics and diaphoretics. Uses: as secondary remedies in acute inflammatory diseases.
- 21. EMOLLIENTS: diminish the force of cohesion between particles of solid matter in the body, by lessening the friction between the particles, especially when the fibers are rigid or distended. Uses: tumors, inflammations, and dryness of the skin.