 DOUGLAS LAMAR JONES
DOUGLAS LAMAR JONES 
Charity, Medical Charity, and Dependency in Eighteenth-Century Essex County, Massachusetts*
THE people of Essex County, Massachusetts, witnessed dramatic changes in the extent and impact of poverty during the eighteenth century. High costs of poor relief, an increasingly transient population of poor people, more complex legal rules for regulating the poor and the dependent, and greater demands for charitable support all became a part of the way of life during the eighteenth century. The Reverend William Bentley of Salem, for one, lamented the passing of the old order when one knew one’s neighbors well and there were fewer “strangers” in town.1 To be sure, life in Essex County had not always been so complex. During the seventeenth century, demographic, economic, institutional, and familial patterns all contributed to low levels of poverty. Land was in relative abundance for the population; families were stable; employment was high; and inflation minimal. By the beginning of the eighteenth century, Essex County—as well as other eastern Massachusetts counties—was disrupted by a rapidly growing population, a declining supply of land in relation to its population, changing patterns of inheritance, migration, inflation, as well as the disruptions of war. Families were forced to adapt to these new conditions of life, and some fared better than others. Some held on to their land; others migrated successfully to New Hampshire; and still others sought employment in commercial centers or as agricultural laborers. But a fourth group presented the people of Essex County with more acute problems: the transient and the residential poor (see Graph 1). As the numbers of the poor and potentially poor increased, charity and the relief of those in need consumed more time and money.2
This essay will examine the policies and practices of medical care for the poor and dependent in eighteenth-century Essex County, a large and populous county which sprawls north of Boston along the coast. Recent historical research on dependency in America by David Rothman and Gerald Grob have illuminated the more general policies of relief, particularly for the nineteenth century.3 The emphasis in this essay will be less on the policies of relief or the “medical” problems of the poor and more on the types of people who required charitable medical care as well as those who provided it. My approach is to use more indirect methods of research—analyzing court records and physicians’ diaries, for example—to reveal how the poor were actually cared for. After first examining religious and legal concepts of charity, this paper will focus on the types of poor people who had medical problems. Next, physicians, midwives, and nurses will be examined, detailing their relationships to the sick poor and the poor relief system.
Perhaps the most basic point to remember about the colonial concept of the “poor” is that it was an all-inclusive category. It embraced not simply those who were economically destitute, although this characteristic was perhaps most critical. But the term “poverty” also applied to dependents such as widows, orphans, the sick poor, and the mentally ill.4 As we think about medical charity, we need to understand that poverty and illness were oftentimes overlapping categories that were not always discerned as separate; rather, the sick poor represented a wide spectrum of people in need of medical care.
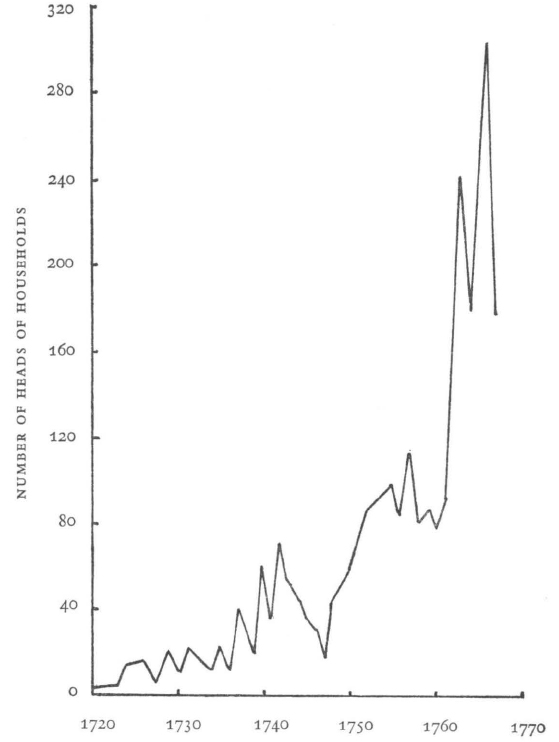
Graph 1
TRANSIENT HEADS OF HOUSEHOLDS IN EIGHTEENTH-CENTURY ESSEX COUNTY, MASSACHUSETTS
Source: Record Books, Essex County Court of General Sessions of the Peace, 1720–1770, Salem, Mass.
Underlying the fact that poverty was a category which embraced a variety of people and conditions of dependency was the Puritan concept of “affliction.” Puritan social theorists—the ministers—understood natural disasters, mortality, disease, and financial reverses as reminders by God that the worldly life was transitory and frail. Affliction was “heaven sent but neutral.”5 Poverty and wealth, then, were an accepted part of the human condition. William Bentley articulated this viewpoint perfectly when he said that “Life with riches is a burden, in poverty distress, when moderately blessed, anxiety.”6 Neither the rich nor the poor were winners because material reward was not to be the goal in life. Bentley, however, did see merit in riches because they permitted people to act charitably: “... many deeds of charity may administer to the wants of the poor: Many virtuous and industrious [people] may be helped into active life.”7
But who exercised charitable responsibility for the poor? In seventeenth-century Essex County, private charity centered around the church. Donations for the assistance of the poor are extremely difficult to measure, and bequests through wills during the seventeenth century were not substantial.8 More importantly, charity was a public responsibility in both the seventeenth and eighteenth centuries. It was not so much that individuals chose not to aid the poor but that taxation provided for their care.
39. Dr. Edward Augustus Holyoke (1728–1829), aged one hundred years and forty-five years. Courtesy Essex Institute, Salem, Massachusetts.
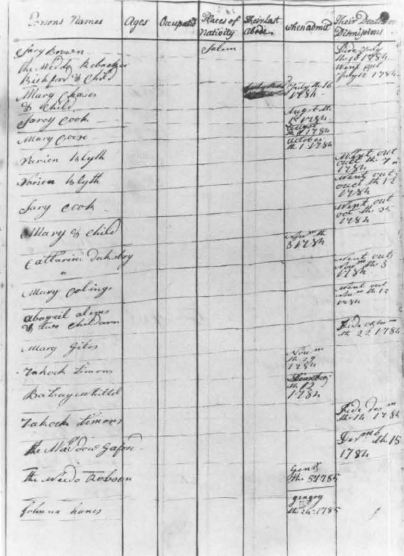
40. List of persons admitted to the Salem Almshouse and Workhouse, 1784–1785. Page 19 of the Salem Almshouse Record, Rules, & Orders, 1749–1798. Courtesy Essex Institute, Salem, Massachusetts.
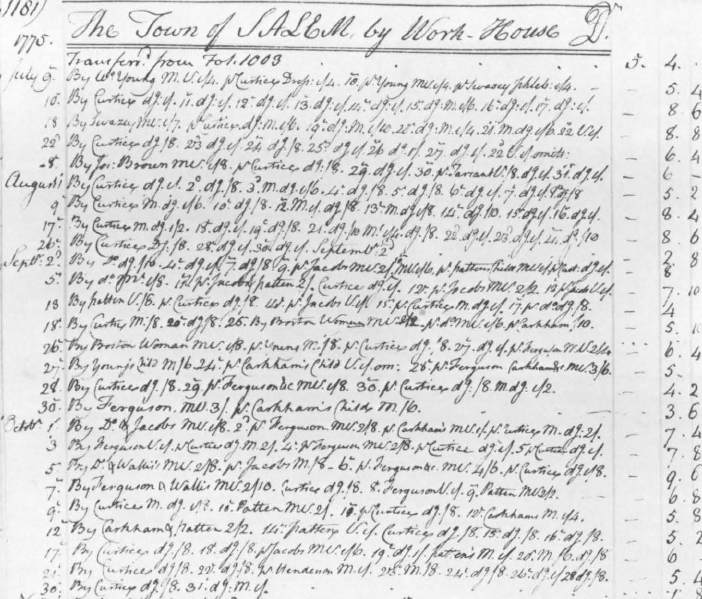
41. Page from the ledger of Dr. Edward A. Holyoke, showing charges to the town of Salem for his professional services at the workhouse. Courtesy Essex Institute, Salem, Massachusetts.
42. Pages from the ledger of Dr. Nehemiah Cleaveland. The right-hand page illustrates payments in commodities and services. Courtesy Essex Institute, Salem, Massachusetts.
43. Pages from the ledger of Dr. Amos Spofford, showing charges to the town of Boxford and payment from the town. Courtesy Essex Institute, Salem, Massachusetts.
Since public relief was the basis of social welfare, Massachusetts distinguished between transient and residential poor people. Resident poor people were supported by the towns in which they had legal residences, and usually were cared for by families within the town. The resident or town poor were an accepted part of the social order in Essex County as well as in other counties in Massachusetts. But as the numbers of the poor and potentially poor increased and as the costs of relief grew, legal requirements for poor relief and medical charity stiffened. Settlement and poor relief laws became more restrictive as the General Court passed new statutes that regulated the presence of transients, limited the towns’ responsibilities for poor relief, permitted towns to warn out nonresidents, and gave towns and courts authority physically to remove any unwanted person. Not until the 1790’s did the General Court rewrite the settlement and poor relief laws in order to reflect the fact that both transients and the residential poor deserved access to poor relief on a short-term basis. The general rule during most of the eighteenth century was that each town had to care for its own poor, regardless of their condition.9
Although the sick poor included both transient and resident dependents, it is important to distinguish among the various types of poor people who received medical care. In spite of the fact that the term “poverty” embraced a variety of kinds of dependents, by examining actual cases of poor people who needed medical care we may refine our understanding of the sick poor. Based on an examination of file papers and record books in the Essex County Court of General Sessions of the Peace, as well as town records concerning poor relief, the following typology of the sick poor was constructed: the ill; the aged; poor women who required public assistance during childbirth; and the mentally ill. While some of these categories overlap (such as illness and old age), medical dependency as well as economic need were the shared characteristics of the sick poor of eighteenth-century Essex County.
The first type, dependents who were ill, was the broadest category, for it encompassed people who suffered from a variety of afflictions such as smallpox, consumption, paralysis, and the injuries of war. Dependents who became ill were likely to contract diseases outside of Essex County if they were transients. Joshua Barker, mustered out of the army in 1760, became ill with smallpox while in the service or shortly after leaving it. Unable to care for himself, he required assistance from the town of Andover until he could be returned to his legal residence in Methuen. Because Barker apparently had no family, he required extensive public support.10
Even the presence of relatives did not insure that the dependent poor could be well cared for if illness set in. Take the case of Abigail Hool. She migrated from Gloucester in Essex County to Portsmouth, New Hampshire, working as a maidservant for Alexander Morrison. But in Portsmouth she became severely ill and was paralyzed. Morrison sent her back to her own family, ending his master-servant relationship and making Abigail a dependent daughter once again. But her own family was near poverty in Chelsea and was unable to care for her. Abigail fell back on her own family when she became ill, and eventually on public poor relief.11
When transients became ill, they often were caught between sparring town selectmen who hotly contested the legal responsibilities of medical care. John and Ruth Pitman, for example, were removed physically from Lynn to Marblehead because the Lynn officials claimed that the couple were legally from Marblehead. While physical removal of the sick poor was not common, it could and did occur. Those who were likely to be removed forcibly were threatening vagabonds and those requiring potentially high medical costs. Ruth Pitman was described as “... very sick and weak[,] not able to Stand and having fitts upon her in the Street....” Without the medical care provided by the town of Marblehead, it was alleged that Ruth would have been in danger of “perishing.”12
Finally, dependents who were ill also included a few surgical cases, arising both from accidents and the injuries of war. During 1776, for example, Dr. Edward A. Holyoke of Salem treated several surgical patients in the Salem Workhouse at the height of the Revolutionary war in Massachusetts.13 Most of the care provided by Holyoke involved changing dressings, as he did with one “Cox,” whose leg was amputated. Dependents who were ill, then, experienced a broad range of diseases and injuries, some of which were contracted within Essex County and others carried into the county by transients.
The second type of dependent with medical problems was the aged. Because of the effects of aging, such dependents were often described as both sick and old. Hannah Long, a transient widow, needed public relief because she was “... a poor and impotent Person and thro Sickness [,] Age [and] Other Infirmities has... been unable to Provide for herself.”14 Widows such as Hannah Long were particularly vulnerable to both poverty and the effects of aging. Mary Flanders, another widow, was poor, sick, aged, and infirm, as were Timothy Parker and his wife.15 With aging dependents, medical care was almost inseparable from economic dependency; the aged poor simply could not always care for themselves.
The third category of dependents were single mothers who had required public assistance at their “lying-in.” For such dependent women, who were often transients and had no relatives nearby, midwives were essential in guiding them through labor. The costs of the birth of children of indigent mothers were all defrayed by poor relief, including the midwife’s fee, food, nurses, and supplies used during the delivery. Because these costs were potentially very high, the General Court provided that the father of an illegitimate child had to pay for one-half of the costs of the lying-in.16 But not all fathers of illegitimate children could either be identified or voluntarily came forward to support their offspring. Mary Harris of Wenham, for example, accused Richard Waite of Brookfield, in Worcester County, of being the father of her child. Waite denied the charge, argued that Mary Harris was a “common prostitute,” and won his case.17 In such cases, the General Court provided by statute that any unmarried woman who bore an illegitimate child could be bound into servitude if her lying-in costs were paid by public poor relief of a town.18
The mentally ill comprise our last category of dependents with medical problems. Although precise definitions of the mentally ill were not commonplace in the eighteenth century, descriptions of these dependents usually included terms such as “idiot boy” and “hardly compos-mentis.” While not direct medical problems from the point of view of treatment, the mentally ill were viewed as dependents in several senses of the word. Widow Joan Reed, for example, required extensive aid from the selectmen of Salem because she was “... very poor and Necessitous and hardly compos-mentis so that she wanders to and fro and is in danger of perishing tho’ there be a small house and about 16 or 17 acres of land though one-half of which belongs to Sd Joan Reed to have it in possession—which she not being capable of improving [sic].”19 Without public charity, Joan Reed would have perished by neglect. Similarly, two young boys, Amos George and Nathan Rolings, required relief because they could not care for themselves.20 While mental illness was not necessarily a treatable disease, those who suffered from it did require—and often received—both public charity and a sensibility that they suffered from more than economic want.
Now that we have identified the types of dependents who suffered from some form of medical problem, let us turn to examine the people who provided health care for the dependent poor.21 At the outset, there were the town officials such as selectmen, overseers of the poor, constables, and coroners who had direct contact with the sick poor. It is important that we remember that these public officials had financial and often supervisory responsibilities for the poor in general and the sick poor in particular. But it was the practitioner of health care who actually provided aid and assistance for specific medical problems. We need not become overly concerned with the distinctions among medical practitioners in eighteenth-century Essex County; those who provided direct health care for the sick poor fell into three categories: physicians, midwives, and nurses and relatives. The relationship of the apothecary to the dependent poor is somewhat unclear, but the poor undoubtedly purchased or were given drugs by apothecaries.
Let us first look at the midwives. As we have seen, midwives participated in the birth of children among poor women, perhaps their most important and persistent contact with the poor. But some midwives also practiced healing by herbal medicines and were the medical practitioners who, before the latter part of the eighteenth century, were commonly called on to examine female patients. This special knowledge of women’s anatomy also meant that midwives had to uphold the moral values of the community. If a single woman was alleged to have had an illegitimate child, midwives commonly testified if confessions of illegitimacy—and the name of the father of the child—were made during labor.22 Midwives, then, were most concerned with one type of dependent: unmarried women. And the midwife’s involvement stemmed primarily from the poor woman’s need for medical attention at childbirth, not illness.
For the day-to-day care of sick or needy dependents, nurses and relatives were common. Usually, families cared for their own members who were sick, but often the poor were migrants or their families were too destitute to provide proper care. The poor relief laws provided that the county court of general sessions of the peace could force family members to care for one another if they were not doing so, and in Essex County, such cases did occur. If no family members were available to provide care, towns hired “nurses” for the sick poor. Both men and women nursed the sick poor, although women seemed more likely to care for women and men for men. Abigail Hool, who was paralyzed, required a female nurse to assist her for almost one full year at a cost of over twenty-five pounds.23 Two men nursed Joshua Barker, the smallpox victim, for several months, receiving cider and pork for their labor.24 Both midwives and nurses received cash and commodities for their care of the poor, usually paid directly by the town. Midwives and nurses, in effect, were employed by the towns to provide appropriate care for dependents who needed medical attention, and the same was true of physicians in Essex County.
But physicians in Essex County had more direct responsibilities for treating a wider range of patients than did midwives and nurses. Indeed, treating the poor was one part of the practice of a physician in Essex County, although the monetary benefits were minimal. But we must remember that physicians, like ministers, accepted the existence of an economically stratified society. In 1720, for example, Dr. William Douglass of Boston distinguished among four types of patients: those who paid an annual sum for medical advice; those who paid by a set fee scale; those (described as “Native New Englanders”) whom Douglass had to bill; and, finally, “others of the poorer sort [whom] I advise and visit without any expectation of fees.”25 Douglass’s description of four types of patients was based explicitly on their ability to pay, suggesting that private charity for the “poorer sort” was provided by some physicians.
From the very beginning, however, physicians in Essex County appeared to have been supplementing their incomes by treating public dependents and receiving payments from the towns. The ledgers and day books of three Essex County physicians—Edward A. Holyoke, Amos Spofford, and Nehemiah Cleaveland—all suggest that their practices routinely involved treating the illnesses of the dependent poor.26 Although these three physicians practiced in different towns in Essex County, they all had a discernible relationship with both the sick poor and town poor relief systems. Indeed, these physicians are particularly interesting because Holyoke practiced in Salem, the major seaport of the county and second only to Boston in population size in Massachusetts, while Cleaveland and Spofford were rural practitioners; Cleaveland lived in Topsfield and Spofford in Georgetown. By examining the practices of these three physicians, we can gain a fuller picture of the role of medical charity in their lives.
Edward A. Holyoke began to practice medicine in Salem in 1749, and continued to do so until his death in 1829.27 While Holyoke was not a typical physician, because of his longevity and his diverse professional activities, he is important to us because he practiced in the major seaport of Essex County and treated many of the poor. The same year that he began his practice, for example, the town of Salem voted to enlarge its almshouse. By 1770, Holyoke had become something of an expert on the almshouse, for he headed a committee which was responsible for building a new workhouse in Salem.28 As Holyoke’s medical practice grew during the middle years of the eighteenth century, so too did his experience with the sick poor. As a physician practicing in a New England seaport, Holyoke could anticipate seeing a broad range of endemic and epidemic diseases. Measles, smallpox, typhus fever, and consumption were all diseases which were likely to be found in a seaport which teemed with new people.29
Because of the attractiveness of large cities like Salem and Boston, migrants tended to collect and become more visible. Formal institutionalization of dependents, whether sick or simply unemployed, became more common as cities built almshouses and workhouses. Even smaller farming towns in Essex County experimented with scaled down versions of the poorhouse, but it was in the cities like Salem that the almshouse flourished during the eighteenth century.30 The first almshouse opened in Salem in 1719, and was enlarged in 1768. Only a few years later a new workhouse was built to replace the old one, and placed on the outskirts of town. Precise numbers of the poor in the almshouse are not available throughout the eighteenth century, but evidence exists for selected years, confirming the growth of the poor population in Salem. In 1749, when the newly renovated almshouse opened its doors, nineteen people entered between December 1749 and April 1750. After the Revolution, in 1787, there were ninety-four people in the almshouse; by the early 1790’s, over one hundred paupers lived there.31
Throughout his career, Holyoke helped to alleviate the problems of poverty in Salem by treating the sick poor. He regularly visited the Salem almshouse, treating the poor. In return for his services, Holyoke received payments from the town, and appeared to have been the primary physician who treated the sick poor in the almshouse until the 1790’s.32 The ledgers of Holyoke’s practice regularly contain entries of the almshouse and then the workhouse. In selected years between 1756 and 1771, Holyoke visited the almshouse between thirty-nine and fifty-five times per year.33 In 1776, he recorded 301 visits to the almshouse. He carefully recorded each visit as he did with private patients, indicating the date of the visit, medication, treatment, and cost.
While Holyoke’s treatment of the sick poor was regular, it did not require a large part of his time; indeed, it was minuscule compared to his regular practice. Early in his career, during the year 1756, he made an estimated 3,500 patient visits. This figure includes repeat visits, and is not an estimate of the absolute number of patients he treated during the year. Rather, it should be understood as patient contact, which averaged about nine people per day. During that same year, Holyoke saw about one poor person per week in the almshouse. The dependent poor of Salem received medical care, in part, because the town was willing to pay for the services of Holyoke. Whether Holyoke also provided medical charity to his own private patients is difficult to say. It is possible that he did, although his ledgers do not reflect whether his patients were charity cases. Holyoke did bill the estates of deceased patients for his fees.
The explanation for the size of Holyoke’s practice among the poor of Salem depends in part on the mortality rate of the poor. Often almshouses were the last refuge for the sick poor, so recovery rates may have been sharply lower in the almshouse than among Holyoke’s general practice. Also, mortality rates among the lower classes were generally higher in Essex County during the eighteenth century than among the wealthy.34 The extent of Holyoke’s contact with poor patients depended not only on the sheer number of dependents but also their ages, their health, and the chances of recovery in an almshouse.
Once they were housed in the almshouse, treatment of the poor followed a typically urban response to public health: isolation, sanitation, and direct involvement of a local physician. The rules of the workhouse, built in 1772, provided that it was to be aired out regularly, bedding and linen changed, strong liquor excluded, the food to be well-prepared, and that upon admission to the workhouse the poor were to “... be free from Lice and foul Distemper.” The overseers of the poor and Holyoke made the Salem poor well if they could, and buried them if they could not.35
When we turn to examine the rural medical practices of Nehemiah Cleaveland and Amos Spofford, we see some of the same outlines of the eighteenth-century physician’s relationship to the sick poor and to the welfare system. But there were differences. The first and most striking difference was in the volume of patient contact; the rural practitioner in Essex County saw far fewer patients per day than did his counterpart in a town like Salem. Early in his career, Cleaveland had 570 patient visits a year compared with Holyoke’s 3,500.36 Both Cleaveland and Spofford saw about ten patients per week. As rural practitioners, they traveled from town to town to see patients, unlike Holyoke who could easily see nearly ten patients per day in the more densely settled Salem.37
Another Essex County physician, Joseph Orne, found that practice outside of Salem was economically and personally unsatisfactory. Orne apprenticed with Holyoke in Salem and then moved to Beverly to set up his own practice. He was apparently modestly successful before the outbreak of the Revolution, but the rigors of traveling to see his patients on horseback, a decline in the number of “Customers,” and his own poor health forced Orne to return to Salem, to escape the “Drudgery of a Country Practice.” At the heart of Orne’s problem was the loss of paying patients: “of those who went away [during the war], many never returned, and their places are now filled in part with Widows and Idlers and Beggars from Marblehead [sic].” Orne well knew from Holyoke that the life of the physician in Salem was better than that in a country town, even Beverly, which was just across the bay from Salem.38
In their smaller-scale practices, both Cleaveland and Spofford had more personalized relationships with the poor and town selectmen. They both received payments for treating the sick poor from towns as a part of the public relief system, but neither had a separate ledger entry for the sick poor as did Holyoke. To Cleaveland and Spofford, the sick poor became more like their other patients, except that payment came in the form of cash from a town. While Holyoke rarely bartered his medical services in Salem, both Cleaveland and Spofford were paid in produce, commodities, and cash. Because their patients were farmers and laborers, Cleaveland and Spofford received flax seed, onions, cabbages, apples, day labor, wood, tobacco, and leather shoes in return for their services. Since the smaller farming towns often did not have almshouses, Cleaveland and Spofford possibly took produce from the near poor in return for treating them. Still, both rural and urban physicians treated the sick poor and were paid by public welfare, whether on the more formalized scale of Holyoke or informally like Cleaveland and Spofford.
In conclusion, medical charity in eighteenth-century Essex County drew upon a variety of people who provided a range of services for different types of the sick poor. Physicians such as Edward Holyoke, in particular, had sustained contact with the sick poor of the Salem almshouse. But rural practitioners also treated dependents, as did midwives and nurses. Whether they provided health care in the busy seaport of Salem or in quiet farming towns like Topsfield or Wenham, those who cared for the poor received payment for their services from the towns. Public poor relief provided the core of medical charity. Well before the “discovery of the asylum” in the nineteenth century, poverty increasingly became a way of life, and medical charity was an integral part of the colonial American social welfare system.