ERIC H. CHRISTIANSON
ERIC H. CHRISTIANSON 
The Medical Practitioners of Massachusetts, 1630–1800: Patterns of Change and Continuity*
CONFRONTED with the formidable task of discussing the highlights of the history of the medical profession in Massachusetts up to 1869, Dr. Oliver Wendell Holmes reminded his Lowell Institute audience that the “medical history of eight generations, told in an hour, must be in many parts a mere outline.”1 Yet, here I am with less than one hour to cover the period 1630–1800, a span of time coterminous with the seven generations of Drs. Clark of Boston that began with Dr. John Clark (1598–1664). Acknowledging his temporal limitations, Holmes expressed more frustration with the paucity of information about his subjects. The hardworking, intelligent country practitioner, he remarked, “more especially deserves the gratitude of his own generation, for he rarely leaves any permanent record” detailing his career. Earlier, in 1853, medical biographer Dr. Ebenezer Alden of Randolph also concluded that the early history of medicine in Massachusetts “is involved in great obscurity.”2 Though hardly obscure, the well-educated and geographically stable Clark dynasty does illustrate some important trends. The general impressions, however, of early medical practitioners suggested by such atypical individuals or families conceal from our view the diverse composition of, and changes in, the profession to which they belonged.
In order to provide a reliable representation of the medical world we have lost, scholars have advised the prospective historian-biographer to provide also an informed social and intellectual context for such an endeavor, thus avoiding the provincial character of most local history of medicine. To achieve balance in such a project requires a discussion not only of the most visible, but also, in the words of Professor Bell, the “hundreds of practitioners in towns and villages . . . who formed the bulk of the profession, provided most of the medical care, and gave the profession its prevailing tone.”3 The need for such comprehensive studies of the identity and demographic patterns of colonial doctors has been recorded in the literature of the field for decades.4 One systematic approach that holds the promise of rendering the obscure more visible and providing balance at the same time is collective biography or prosopography.5
Collective biography requires many kinds of sources already familiar to demographer and historian alike: the histories of towns, counties, and institutions; vital data; church registers; and court records. In addition to these sources, for this paper a computer permitted further exploitation of techniques developed by historical demographers to reconstruct families down through the generations and by social historians to analyze town and group characteristics.6 With these aids, the researcher can develop perspectives based on more representative data than could be compiled otherwise. Unfortunately, the limits imposed by time and by the titles of other papers in this symposium prevent detailed discussion of many biographical and demographic characteristics of this paper’s subjects. While Holmes complained about the dearth of information concerning early American doctors, he did not conduct an extensive investigation of then available records. The rich sources mentioned above provide much information for an in-depth study of colonial doctors. With the partial reconstruction of their lives complete, it is possible to study over time the increase of doctors, the patterns of individual and group distribution, their educational experiences, and some of the possible effects of these features on the organization of medical practice.
scope, qualifications, and definitions
An important objective of this study is to determine with some measure of certainty the number of practitioners throughout the state at different times. In such a study one could argue for the inclusion of all mothers and fathers as part-time practitioners, for, indeed, the family assumed the immediate responsibility for the health of its members. One could also assume that all ministers exhibited the “Angelic Conjunction”—the healer of spirit and body—but I have included only those noted in the records for their expertise.7 Most medical men were readily identified by their titles. Herein lies the principal reason for the omission of female practitioners. Vital records of towns and the like rarely mention “midwife,” “doctoress,” or “nurse” before the names of women who might have acted out the functions of one of these three categories. As Professor Jones demonstrates elsewhere in this volume, court records promise to help determine the identity of female practitioners, who remain most elusive subjects for study.8 Unlike urban Britain, which also experienced change in this regard, but resembling the customs in the provincial towns, the basis of separating “physician,” “surgeon,” and “apothecary” proved inoperative in the colonies as early as the 1620’s.9 Even with the advent of such agencies of urban culture as The Boston Directory in 1789, this nomenclature did not usually correspond with the appropriate British function. In effect, these conditions produced a hybrid, a general practitioner, a “physician,” some of whom also had expertise in a specialty like surgery or obstetrics.
“It was not customary,” wrote Dr. Samuel A. Green in 1881, during the colonial period “to address or speak of a physician by the title of doctor ... perhaps because so few had diplomas.”10 His use of the term “physician” reflects both late nineteenth-century definitions as well as the nomenclature of the British medical hierarchy throughout the colonial period. To his knowledge, the earliest date at which the appellation “Doctor” appeared in Massachusetts is 1668. And yet the logbook of the Mayflower in 1620 indicates that Samuel Fuller was “Dr. Fuller,” although he did not have a diploma either.11 Not until the proliferation of medical schools during the nineteenth century granting thousands of diplomas did “physician” become generally equated with the recipient of the M.D. Nowhere in colonial America did there exist effective restraints on the use of the title of “Doctor” or uniformly accepted qualifications for who could practice. Not all of the contents of “this attic full of institutions,” as Daniel Boorstin describes the formal agencies of the English medical hierarchy, were involved in the transit of culture to the New World, but early settlers were certainly aware of them.12 Dr. John A. Raach points out that most New Englanders immigrated from English counties, such as Norfolk, Suffolk, and Essex, with a high concentration of M.D.’s and men with other types of formal training.13 The first groups coming to New England sought to avoid the disaster of Jamestown by including individuals with skills necessary for a successful community, like male and female practitioners who would provide health care for a rural, working-class society. And in an environment that encouraged multiple careers, virtually all doctors were engaged also in other income-producing activity.14
Nearly two-thirds (874, or 63.8 percent of the 1370 during 1700–1792) of the men either styled themselves or were referred to in the records as “Doctor.”15 In England at that time, for example, Peter Laslett observes that some parish clerks and ministers “were more generous in distributing titles to their entries and it would be foolish to expect any rigorous consistency.”16. My findings, however, suggest that, with more than marginal consistency, the use of titles in the colonies, where their availability to ordinary people was limited and highly prized, even the title of “Doctor” was perhaps considered by many to be preferable to no title at all. The freedom with which these men employed, and were granted, the title of “Doctor” is one important reason that this study seeks to include as many as the records reveal. Only then can we appreciate the action of reformers, who, after 1750, would focus much of their effort on the indiscriminate use of the title “Doctor.” For the period 1630–1800 nearly 1600 doctors were identified from a wide variety of sources, both printed and archival. The primary focus is on the 1370 medical inhabitants of some 268 Massachusetts towns and eleven counties during the period 1700–1792.
growth
The richness and accessibility of the state’s early historical records yield an unanticipated number of doctors exhibiting, as a group, an equally impressive rate of growth. During the period 1700–1790, the number of doctors increased by 32.4 percent every ten years, while the general population increased by only 24.3 percent over the same interval. Throughout the seventeenth century the ratio of doctors to population remained stable at about 1:1,000. But because the subgroup of doctors doubled more rapidly than did the general population over the next century (26.8 years for doctors and 37.4 years for the total population), the ratio increased steadily from 1:1,000 in 1700 to its high of 1:417 in 1780.17 And though comparisons with other areas are employed with much reservation, the figure for 1780 might indicate that in Massachusetts, among all states, we find the highest concentration of medical men.18
Since the 1870’s, researchers have come to rely upon Dr. Joseph Toner’s estimates for the number of practitioners during the American Revolution.19 Assuming the population to be 3,000,000 in 1776, Toner suggests the figure of 3500 doctors with a ratio of 1:800 [1:857]. In 1960, Professor Shryock arrived at a ratio of 1:600 based on a smaller population of 2,000,000.20 Using either approximation, or the mean figure, in 1776 Massachusetts contained about ten percent of the population, and with 643 doctors, nearly twenty percent of all doctors in the new republic.
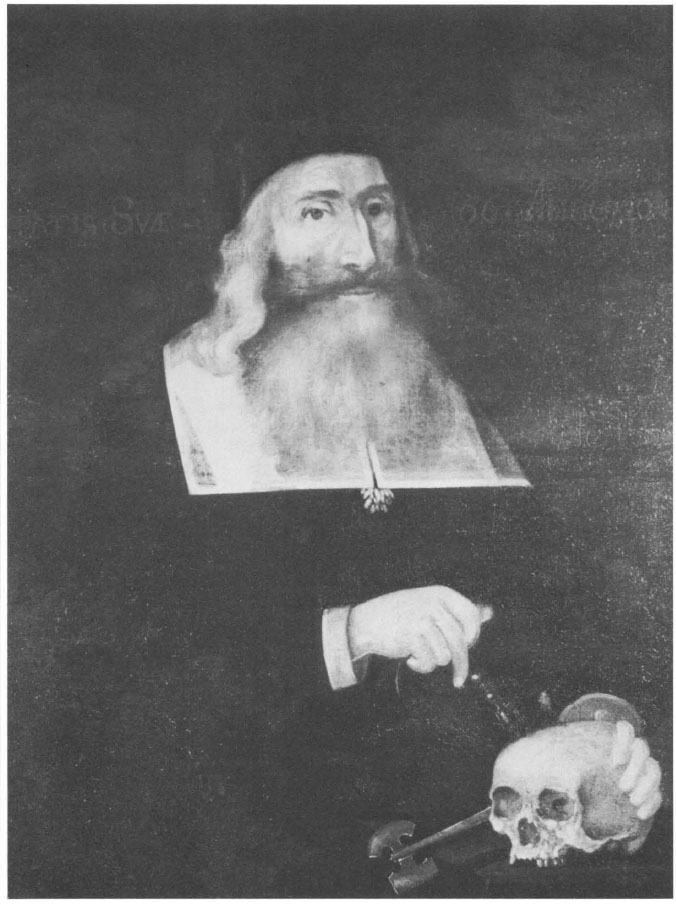
1. Dr. John Clark (1598–1664). Painted in Boston about 1664 by Augustine Clement or his son Samuel. Courtesy Boston Medical Library.
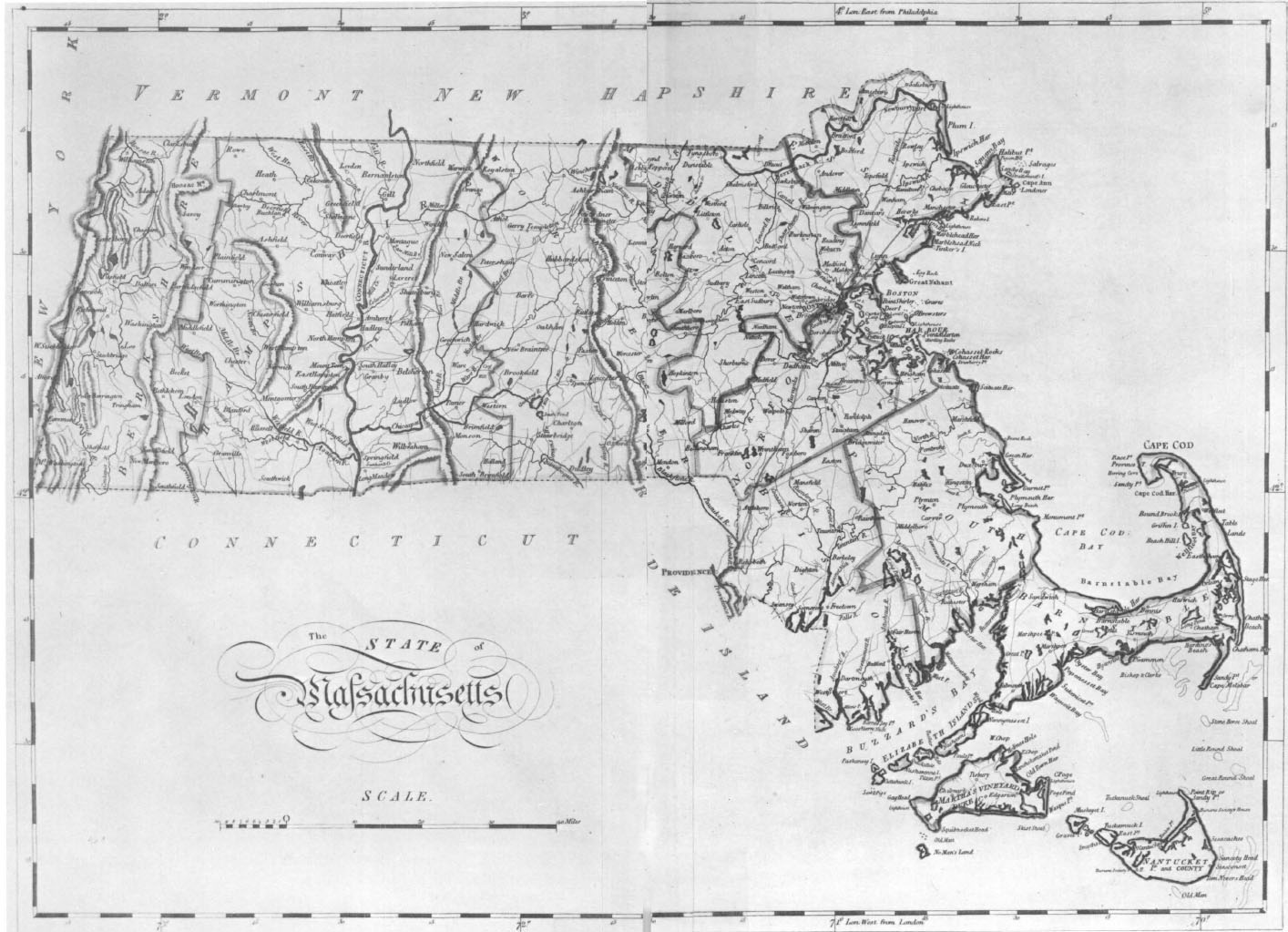
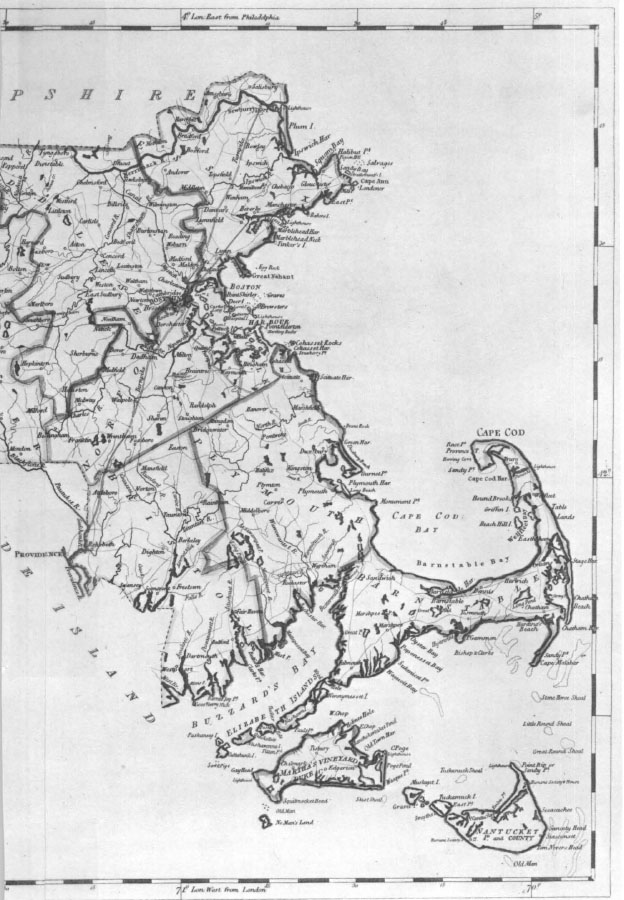
2. Map of Massachusetts in 1800, showing the counties. Franklin and Hampden Counties were not created until 1811 and 1812, respectively. From Carey’s General Atlas (Philadelphia, 1816). Courtesy Harvard College Library.
3. Articles of Indenture of Joseph Lemmon, Jr., to Dr. Zabdiel Boylston of Boston, 18 May 1736. Courtesy Boston Medical Library.
4. Letter from Dr. Cotton Tufts of Medford to Dr. Joseph Warren in Boston 22 July 1774. Tufts seeks Warren’s advice for relieving rheumatic pains in a boy of twelve or thirteen years of age. Courtesy Boston Medical Library.
5. Dr. Cotton Tufts (1731–1815). Painted by Benjamin Greenleaf in 1804. Tufts was apprenticed to his brother Simon in Medford. He began to argue for the establishment of a state medical society in 1765, and, after it was organized in 1781, Tufts served as its fourth president, from 1787 to 1795. Courtesy Boston Medical Library.
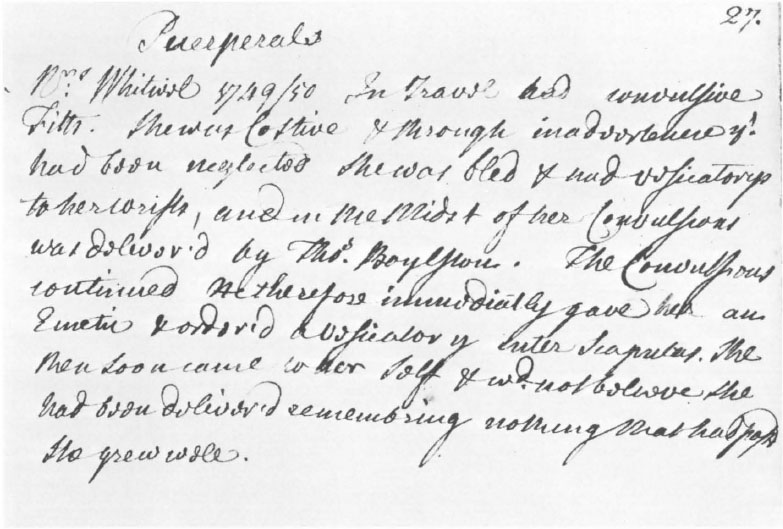
6. Clinical notes of Dr. John Perkins (1696–1781). This 1750 note concerns the successful treatment of a woman who had convulsions at the time she delivered her baby. Another physician, Dr. Thomas Boylston (1715–c. 1771), served as her obstetrician. From Perkins’s unpublished ms “Observations Medical & Chirurgical.” Courtesy Boston Medical Library.
According to Toner, the geographical distribution of the 3500 doctors in 1776 produces a ratio of 1:800 for the cities and 1:1,000–1:1,200 in the countryside. There are several observations claiming an “urban surplus” of doctors, but Toner argues that all ratios are probably too high because so few towns had populations greater than 5,000. Once certain occupational thresholds are reached, towns with populations as small as 1,000–2,000 should also be considered “urban.”21 So for the present study an arbitrary selection of towns with more or less than 1,000 inhabitants in 1765 and 1790 produces results that conflict with earlier estimates.22 For example, in 1765 the ratio of doctors to population in towns over 1,000 in 1:1,035, rn the smaller towns 1:557. And the results for 1790 are nearly identical: for towns over 1,000 the ratio is 1:954, and for smaller towns it is 1:588. There were, of course, cities with more than 1,000 with high ratios in 1790, like Great Barrington in Berkshire County (1:683), Easton in Bristol County (1:488), Worcester (1:419), and Boston (1:563, almost the same as in 1765). For Massachusetts, at least, country towns probably contained more medical practitioners than the cities. The ambiguous nature of a “surplus” or “shortage” of doctors will be discussed later. With these general characteristics of the doctor population as background, we can investigate other features of the observed growth patterns, specifically their origins, distribution, and educational experiences.
other features of growth
As might be expected, Europe produced less than ten percent of all colonial Massachusetts practitioners. The great migrations of the seventeenth century, however, contributed almost one-third of the early-period doctors, while only 3.9 percent were Europeans by birth during the next century.23 The geographical mobility in the decades following the initial settlement of New England is indicated by fifty-three doctors in the later period who immigrated from bordering provinces.24 With immigration high after 1750, nearly ten percent of the state’s doctors were recent arrivals in search of patients.
Among the native-born, most were from the eastern counties that were more densely populated and consistently produced more medical men than the developing regions of Worcester, Hampshire, and Berkshire; Suffolk, Middlesex, and Essex together account for one-half of the 1370. Regardless of time or location, one-fourth of the medical inhabitants of the counties came from other Massachusetts counties or from outside Massachusetts. Doctors seem to have been less geographically stable than the general population, and their movement as a group after they started to practice reached thirty-four percent; by 1760 one-quarter (24.2 percent) of this mobility was among counties. Dr. Giles Firmin, perhaps the first practitioner to note the social impact of this instability, complained to Governor John Winthrop in 1639 about those who “range from place to place on purpose to live upon the country.”25 Those men without apprenticeship experience or college attendance moved throughout the century significantly more often than did their trained counterparts.26
For the entire 170-year period, no more than twenty-five percent (421/1,600), attended college, received a degree, or attended lectures in Europe, New England, or another colony. But after 1750 Harvard and Yale college graduates found medical practice much more attractive than earlier in the century (26.1 percent increase).27 This trend reached its peak also in the 1760’s when forty-six percent (71/153) of all the beginners had attended college. Indicative of rapid growth within the ranks of the college graduate doctor is that 46.9 percent of all graduates who entered medicine did so between 1751 and 1780.
Similarly, less than one-third of all doctors during the period 1630–1800 served apprenticeships of at least one year’s duration, but during the eighteenth century almost thirty-six percent (488/1370) were apprentice-trained, an increase of twenty-six percent over the previous century. Consistent with other changing patterns, after 1750, apprentice-trained men increased by twenty-eight percent relative to the earlier period. In spite of their numerical strength, these men were never to comprise more than one-half of all beginners in each decade. A college education or a preceptorship represented but two of a large selection or combination of possibilities. Most of these categories of experience, however, such as inoculating in a smallpox hospital, acting as surgeon or surgeon’s mate in a military campaign, or caring for the needy in the poorhouse were virtually closed to those without a degree of some kind or apprenticeship experience.28 Granted, these experiences are rather limited prior to 1700, but one agency of practical experience, the medical family, provided training throughout the colonial period.
Recruitment from within the ranks of the professional family accounts for a substantial number of the 1600 doctors during 1630–1800. Of the 149 seventeenth-century doctors, seventeen percent were joined and then succeeded in practice by one or more sons. In the eighteenth century nearly twenty percent (271/1369) of all practitioners either came from (15.7 percent), or married into (4.1 percent), medical families. Within this group with medical fathers we encounter the dynasties, the fifty-two families, including that of Dr. John Clark, who perpetuated the traditions of the healing arts for three or more generations. The appearance and distribution of multi-generational medical families is similar to the patterns for the larger group. For example, over one-half (fifty-eight percent) of the 215 with medical fathers flourished in Essex, Middlesex, and Suffolk counties, and nearly two-thirds (63.4 percent) first began to practice after 1750, with the per decade high during the 1750’s, when they constituted almost one-fourth (33/133) of all the beginners.
Unlike the larger group of medical men whose fathers were not also practitioners, families of three or more generations of doctors were geographically stable and well trained. In the older counties like Middlesex, where the general mobility of doctors might reach forty percent after 1750, or the rapidly developing newer counties such as Berkshire, created in 1761, where mobility surpassed eighty percent, the mobility rate for the multigeneration group rarely exceeded fourteen percent. While fewer medical family doctors attended college than the larger group, all of them were apprentice-trained, which means that forty-four percent of all the apprentice-trained were members of medical families. In these families, fathers provided in lieu of college credentials practical training for their sons and bequeathed to them land, medical supplies, books, and a ready-made clientele. These kinship and professional ties provided adequate protection for years, and they seem to have grown stronger when challenged by an ever increasing number of mobile itinerants.
Medical families or dynasties exhibit features similar to the larger groups of apprentice-trained and/or college-graduate men, primarily voluntary geographical stability or calculated movement (which usually brought them back to the towns of their birth), and a high incidence of apprenticeship training, then the predominant form of professional education. Relationships established through family ties and educational experiences also produced an informal network of communication between similarly qualified or like-minded individuals living miles apart. News concerning the job market passed quietly within this tight-knit medical patronage system. After 1750 the infiltrations of the rapidly expanding group of mobile interlopers into this network had important implications for the strategy and effectiveness of medical reformers well into the nineteenth century.
implications
In the last few years, scholars, including Professor Brown, have argued that the modernization of American society gained momentum after 1760.29 Processes of change long at work, and later accelerated by the events of the Revolutionary era, produced a breakaway from some traditions and a reaffirmation of others. Alarmed by altered surroundings, some contemporaries warned others of the possible loss of close personal ties and the virtues of rural life. And, like the experiences of other groups in this pluralistic society, tensions between coexisting and often opposed forces of modernization and tradition within the medical profession were accentuated also by changing economic and demographic realities.
A changing environment in which shortages of available land, uncertain opportunities, and multiple careers were common might have stimulated “upwardly mobile, achievement-oriented” individuals to try their hand at doctoring their neighbor’s complaints after home remedies had failed or if the local doctor was unavailable.30 Unwilling to have their career choices limited by regulations or time-consuming and expensive training, these individuals displayed little deference toward their betters. One alarmed observer noted the strained economic conditions and dislocation of people in Massachusetts following the Treaty of Paris in 1763. As a result of these circumstances, he added, more men were unemployed, and “having poor Stomachs to return to the Stall or plough from whence they came; some of them commence quacks and call themselves Doctors.”31 With the vast majority of doctors coming from nonmedical families, especially farming, and with less than ten percent of them sons of men with college educations, it seems reasonable to assume that medical practice was an attractive alternative to the sons of those farmers who did not have enough land to distribute among all their offspring, and who could not afford either to send them to college or to pay apprenticeship fees, or who refused to do so.
Apprenticeship instruction had long been the most traditional form of training apothecaries and surgeons in England and her colonies even in the presence of expanded educational and career opportunities. Some scholars have identified conditions in America that they feel contributed to the declining vitality of this pedagogical technique during the eighteenth century. Among these writers, Bernard Bailyn did not restrict his analysis to the apprenticeship patterns of any particular occupational group, but concluded that generally “evidence of its decline was as clear in its internal characteristics as it was in quantitative decrease.”32 Such a decline is attributable to a societal tendency to transfer the burdens of some vocational training from within the home to external agencies. To apprentices, he argues, the old obligations to formal training were “archaic entanglements,” obstacles in the path of independence. To its defenders, the substance and function of the medical apprenticeship indeed experienced flux, and its prospects were unclear, but not futile. Another writer suggests that the war of the American Revolution weakened the system as regularly trained men entered medical service to treat soldiers and sailors, only to be rivaled in their absence by the untrained intruder answering the demands for medical services;33 even some Tory doctors were allowed to remain.34 During the 1770’s a large number of untrained beginners did appear, for in that decade we find 219 men first starting to practice (sixteen percent of 1370), of whom only forty-two percent had served at least an apprenticeship. But the results of the present study reveal that in spite of the documented intrusion of untrained practitioners into temporarily vacant practices (and most were forced to leave once the absent incumbent came home from war), the apprenticeship system for medicine grew stronger, not weaker, in the eighteenth century.
A demand for medical services certainly did exist, whether or not the practitioner had credentials, throughout the colonial period, and such conditions encouraged some to seek access into the medical profession via traditional means, while others skipped the formalities, and, to paraphrase Tammany Hall sachem George Washington Plunkitt, they “seen their opportunities and they took’em.” Town selectmen actively sought resident bone-setters, midwives, and physicians, and offered subsidies of land and/or money to those who promised to “[live] among us Some years.”35 True, the wandering individual, male or female, or uprooted family was always suspect of becoming a burden to the town’s taxpayers, but in these circumstances a mobile doctor regardless of training might not have been unusual or socially undesirable.
The mobility of self-taught doctors, one source of their obscurity in the records, suggests that frequent movements represent ventures not of success but of repeated failure to compete successfully with established and trained counterparts.36 This movement is documented well into the nineteenth century.37 Before 1800, physical dispersion and smaller average size of communities in America, argues Daniel Calhoun, allowed a “large proportion of doctors to enjoy a monopoly on practice” in some communities.38 If not a monopoly, some doctors did enjoy a thriving practice, but long before the turn of the century they evidently could not meet the needs of all the potential patients in the community. Even today, observes Rashi Fein, with legal restrictions on medical practice, there exist no wholly acceptable criteria for an “oversupply” or “shortage” of medical personnel.39 The respected doctor could create a demand for his services as healer and preceptor, but for early Massachusetts or colonial America as a whole we have perspectives only on the ability of the population to consume his services. With widespread demands for medical services on record, it might be imprudent to conclude that because of their mobility or large numbers a “surplus” of doctors did exist.
Even in the presence of a flourishing self-doctoring tradition in early America, and the willingness of towns to attract resident doctors with varying degrees of skill and experience, those with a proven commitment to learning, and with at least the potential of contributing to the stability of the community, would receive their deference and prevail over the less-polished and self-taught.40 Seen, however, from the perspective of the geographically stable and trained men in towns and cities, something had to be done, wrote one defensive Dedham practitioner in 1764, to “prevent the intrusion of every ignorant drone that assumes the title of doctor” into their ranks.41 The tone of his remarks signals a jolt, a discontinuity, a realization that what had worked in the past to control competitors might not work in the future. A major issue of strategy for such reformers, the conservators of tradition and arbiters of change, became how they could best suppress “this Herd of Empiricks who have heaped such intolerable contempt on the Epithet Country practitioner.”42 Their concerns would not develop into a general social campaign against untrained mobile doctors, but rather an intragroup clash for local control and legitimacy.
As cracks appeared in the structures of the deferential social order (what some recent studies refer to as an “ascriptive” social order), many groups sought to strengthen its weak points, others to create another order based on acquired expertise. In the decades after 1760 the altered milieu brought forth political parties, county bar associations, interest groups seeking protective legislation for their members, societies offering restricted membership to those who wished, according to Professor Cassedy, to “be or act as learned men,” and voluntary associations created by reform-minded individuals.43 Even with a growing, more concentrated population, and the spread of urban culture throughout the area, the vestiges of an isolated world-view persisted. Most of the groups, especially the voluntary associations, which included medical societies, achieved their goals more effectively at the local, rather than at the state or national, level.44 And while the rhetoric of republicanism indeed stimulated the formation of groups dedicated to national purpose and to the completion of the unfinished revolution, its phrases and ideals also elevated the individual to new levels of self-esteem; a nation of individuals might oppose the formation and activity of restricted groups whose very composition and intent ran against the grain of individual rights. In these circumstances the health of individuals and their right to be protected from alleged incompetents became an issue that doctors tried to support themselves, although they did not try very hard to secure legislative sanctions.
Perhaps united only by disputed titles and qualifications for practice, doctors composed not one group but many—some that shared communalities of interest and background yet espoused conflicting goals. Granted the existence of overlapping membership, multigenerational medical families and apprentice-trained or college-educated doctors tended to offer solutions to problems that would preserve their own self-interest. The appearance of new institutions, such as the Massachusetts Medical Society in 1781 and the Harvard College-Harvard Medical School connection after 1783, were received with ambivalence throughout the state.45 Those who had relied upon the apprenticeship system for local control might balk at the possibility of basically academic qualifications for practice and a centralized medical authority in Boston. Doctors near to, and distant from, Boston would argue with the state society during the 1780’s and 1790’s for the right to determine on their own the appropriate duration of the apprenticeship in order to promote response at the local level.46 Local groups tended to overestimate the strength of the Boston medical establishment, which itself was experiencing a bitter controversy between the state society and the new medical school at Cambridge. And while many desired to expand upon the basic virtues of the apprenticeship as a medium of self-improvement, doctors in the most rural areas began to acknowledge that the system was itself, because of the insularity of the pupil-mentor framework, rather limited as an educational tool or agency of control over entry into practice.47
Emerging from long-existing relationships between mentors and pupils, generations of family ties, and colleagues in practice, county medical societies like the Berkshire Medical Association created in 1787 or the Middlesex Medical Society in 1788 also restricted membership largely to medical men, but offered the practicing self-taught doctor an opportunity to improve himself by associating with trained men and their pupils.48 Lectures would supplement the basic pupilage for those who could not travel to Boston or Cambridge, and these local societies certified their own pupils. The intense bickering and one-upmanship that plagued Dr. William Douglass’s efforts to create a stable Boston Medical Society in 1735 would have to be overcome by more realistic attempts based on compromise as well as commitment to improved medical services.49 Such realistic arrangements, argued Dr. Benjamin Waterhouse in 1791, would best promote the the interests of the Faculty by reducing destructive bickering among doctors and improving the general level of practice.50
Inclusive local societies would act as a buffer between the extremes of rampant individualism and centralized or distant control. The primary purpose for creating the limited membership state society in 1781, complained one western member-correspondent, had been to eliminate the untrained doctor; but the efforts of the Massachusetts Medical Society had not by 1784 in “the least degree prevented the Increase of Empirics.”51 Perhaps Calhoun is correct in observing that immigrants to larger towns and cities knew or remembered local isolation as a standard even while “they sought to work out a life appropriate to the city.”52 Yet medical immigrants to larger communities, or those who grew up in them, also sustained their bickering in new surroundings. Respectability for the profession, declared an orator in 1787 to the members of the Berkshire Medical Association, “could never be attained so long as we are activated by the meanness of jealousy and opposition to each other.”53. Even with modest hopes for the future success of their efforts, local groups recorded Pyrrhic victories and the state society would, by 1803, be forced to reevaluate its tactics and to expand its membership to represent more realistically the demographic realities of medical practice in the state. In these circumstances we can better understand why some reformers were frustrated and driven to define the self-taught as adversaries, as if “to vindicate their own uncertain worth by assaulting those around them.”54. Only in the distant future would the medical profession achieve that collective individualism expressed as “You are as good as I, and let us help one another.”55
The medical settlement of Massachusetts was essentially over by 1790, though not every town could boast of a resident doctor, but demographic and social realities had decentralized medical authority and training throughout the state. True, the American Revolution had brought together men of varying degrees of experience and had inspired them further, but these changes were set in motion during the 1750’s. A balance between control and personal freedom would, in these circumstances, produce a tenuous compromise at best. These eighteenth-century developments established a framework for the clash between sectarians or regulars and proprietary or college medical school graduates so characteristic of the following century.56. There was both change and continuity in the composition and organization of the medical profession during 1630–1800. But the inertia of traditions and the apparent success of the self-taught doctor reduced the options available to medical reformers in their responses to a more rapidly changing social and intellectual context.