 G. B. WARDEN
G. B. WARDEN 
The Medical Profession in Colonial Boston*
FOR better or worse, large organizations dominate modern life. I Business corporations and the bureaucratic state have received a justifiably large amount of analytical attention from scholars in many disciplines, like Marx, Durkheim, and Weber.1 Such institutions seem so much a part of our existence that many people may tend to think that their creation and development were parts of some inevitably determined plan. It is worth remembering, however, that until the last hundred years most societies and cultures managed to get along rather well without the large public or private institutions which we now take for granted. Parkinson’s Law may help to explain how such institutions develop after they are created, but the exact nature of their origins remains obscure.
The historical origins and development of professions and professional associations as specialized, institutionalized, occupational organizations suffer from comparable difficulties of being taken for granted, of appearing to be almost inevitable, and of being only inadequately investigated. In colonial America the organization of churches and of the clerical profession has received the most scholarly attention.2 Colonial lawyers and the legal profession in its primitive years have been studied, although with somewhat inadequate results.3 We know a great deal about early American craftsmen, cabinetmakers, painters, printers, and silversmiths but little about their organization or associations until after the dawn of the nineteenth century.4 Somewhere in the middle are studies of individual scientists and early scientific organizations, of which physicians would seem to be a part.5
Other scholars at this conference will provide information about early medical practice, medical literature, medical education, and the contributions of individual physicians. My present purpose is to explore some speculations about medicine and physicians in the social, economic, political, and intellectual context of colonial Boston. Some of the following speculations may be very familiar to those who specialize in the history of colonial medicine, or very obscure, given a meager knowlege of technical details. My aim is to explore some of the nonmedical elements of the medical profession in early Boston.
In the usual sort of inquiry of organized institutions, the usual questions to start with would probably be how and why the medical profession began and developed. Answering such questions would produce some rather predictable information; such a conventional approach strikes one as pretty obvious, one-dimensional, uni-directional, semi-hagiographical, and not really very interesting. A slightly less conventional approach is to ask instead how and why the medical profession did not begin and did not develop in early Boston. Many people, of course, do not like such a counter-factual approach, and others would quarrel with its basic premise by pointing to the work of individual physicians, organized efforts during Boston’s many inoculation controversies, medical literature available in the town, scientific and medical education at Harvard, and other elements showing convincingly that in fact a medical profession was beginning and was developing in colonial Boston.
All that is true, of course, but it would be equally hard to argue that the medical profession, training, literature, and education were as well organized as the clerical profession, printers, politicians, and, in the late colonial period, lawyers. Given all we know about medicine in Boston, the question still remains why physicians were not as well organized as other professions at the time, or as the medical profession itself became in the early nineteenth century. Phrasing the question in that fashion opens up some intriguing possibilities about the place of colonial medicine in the context of not-so-obvious legal practices, demographic trends, social patterns, family life, economic developments, and public policy, which specialists in medical history may need to know about from conventional historians.
If we look at the medical profession as other analysts have examined the salient characteristics of specialized, organized, institutionalized, public or private groups in the modern era, it becomes a little clearer what the medical profession needed in order to develop and what it did not have in the colonial period. Among those characteristics we may include the requirements of state subsidies and sanctions, monopolistic privileges, limitations on legal liability or accountability, favorable conditions of economic supply and demand, regular sources of reliable information, tribalistic protection of craft secrets and mysteries, graduated standards of competency to create institutional hierarchy, exclusion of amateurs, specialized technical knowledge (preferably in a quasi-secret language), specialized self-consciousness of the group and its members, internal rather than external procedures for distributing rewards and assuring compensation, and, of course, pretensions (real or imagined) of social utility. All of these characteristics distinguish the modern corporations, bureaucracies, and professional associations, as well as earlier forms of corporate organizations like the clergy or medieval guilds.
It would be impossible to go into each of these characteristics in great detail as far as physicians in early Boston are concerned. Instead, some of the limitations on professional organization of physicians involving law, demography, social attitudes, public finance, and politics as they pertained in the town will be emphasized.
The legal limitations on the medical profession in colonial Boston, oddly enough, concerned three matters familiar to modern doctors: licensing standards, malpractice, and fees. Like all other groups in early America except the church, doctors faced an insuperable handicap in any attempt to organize themselves in corporate fashion. The usual attributes of incorporation could be established only by royal charter, and after 1688 it was likely that England’s Parliament would also have a hand in any grant of corporate privileges. As in the control of colonial commerce, manufacturing, and banking, there was little chance that any colonial group of physicians would be able to receive royal or Parliamentary approval in competition with the official monopolistic powers already granted to the Royal College of Physicians and the English universities. As long as the English monopoly prevailed, colonial physicians who were dissenters would have to resort to the Scottish universities for medical degrees or simply practice without educational requirements or corporate status.6
Unwillingness to grant corporate, monopolistic privileges to groups like colonial physicians was not simply royal policy. It was also a stubborn impediment in the attitude of colonial political leaders as well. The disapproval of local elites in Massachusetts thwarted schemes for incorporated banks, and local leaders adhered to the traditional Whiggish antipathy toward standing armies. It was thus unlikely that local legislatures would grant corporate monopolistic privileges to any group other than a church; even educational institutions at the college level could not expect easy legislative endorsement. In Boston itself, the resistance to corporate privileges was a matter of popular feeling rather than elite resistance; in town meeting the voters generally refused to adopt even vaguely restrictive market regulations in traditional fashion or to allow the selectmen to have corporate dinners at public expense.7 Except in religion, the general antipathy to corporate privileges meant in effect that doctors would not be able to receive public sanction for corporate organization, a prime ingredient of professional association.
Official sanction, of course, is not the sole determining factor in the origin and development of professional organization. Informal, unofficial groups could and did flourish without being approved in public fashion. But as long as full legal privileges were withheld from the doctors, their organization and influence as a group might be no more than those of merchants chatting on the Exchange or dock-workers grousing at the local tavern, and much less than the clergy in synods or consociations.
The absence of any grant of self-regulating privileges for doctors by legislative or executive charter of incorporation would have left the incipient medical profession as a private association. As a result, it would have been difficult, though not perhaps impossible, for the associated physicians to get legal sanctions from the courts to collect dues, to set standards of practice, to exclude interlopers in the field, to enforce agreements as to fees, and to chastise erring members. Moreover, as a private association without corporate status, any organized group of doctors in the colonial period would have been liable as individuals for the total expenses or debts that the group may have incurred, much like a private partnership in its older forms, in the absence of any express stipulations to the contrary.
That financial problem may not have been as crucial in the difficulties limiting the development of the medical profession as the more familiar problem of liability for negligence and standards of care imposed on the medical practitioner. Indeed, insofar as we can speculate from meager hints about the subject in the colonial period, the problems of liability may have been a primary hurdle in any individual’s decision to follow a medical calling in the first place, as well as the ability of medical practitioners as a group to associate and set standards of practice. Without corporate limitations on liability, doctors, surgeons, and apothecaries were on their own as isolated individuals and as self-insurers for any damages from negligence or contractual breaches. Moreover, if what appears to have been the English standards as to surgeons applied in the colony, medical practitioners fell into the category of common callings from which a higher standard of care and strict liability were expected. That is, anyone pretending to have the skills of a physician would not be allowed some of the ordinary mistakes or lapses in judgment that practitioners in other occupations may have enjoyed. Moreover, in the absence of any disclaimer to the contrary, any physician undertaking to effect a cure would be liable for breach of contract if the cure failed. In the absence of any incorporated hospitals during the period before charitable immunity developed, the doctor faced some severe legal handicaps in the ordinary course of his practice. In actual practice, however, the higher standard of care and strict liability imposed on physicians at the time meant in practical terms that they simply would not undertake any risky practice and would expressly stipulate with a patient that no cure was guaranteed.8 Still, the legal standards of liability in that early day provided very little encouragement for a would-be doctor to follow such a risky calling and positively discouraged any high degree of experimentation in broadening the scope of medical activity.
The legal impediments for the individual doctor and medical profession did not stop with the absence of incorporation and with standards of strict liability. There was also the matter of the physician’s ability to collect a fee and even to specify the amount of the fee. In the eighteenth century Boston suffered simultaneously from a long economic depression and before 1750 runaway inflation of the local currency.9 Physicians were of course not alone in the problems of balancing their accounts. But during the frequent epidemics and general mortality conditions of the period, doctors faced rather severe problems trying to collect fees from those who survived their cures and especially from the estates of those who did not. Lawyers in time developed the practice of requiring a bond or mortgage from a client in advance for legal services, but physicians naturally had little chance to take advantage of such a device.
20. Judge Samuel Sewall’s account with Dr. Zabdiel Boylston. Mrs. Sewall’s illness, which necessitated bleeding on 9 May 1718, is not mentioned in her husband’s diary, but two years later her sudden death, which followed “a rising of Flegm that obstructed her Breathing” within an hour, was a “great astonishment.” Massachusetts Historical Society Collections, series 5, vii (1882), 254–255. Courtesy Boston Medical Library.
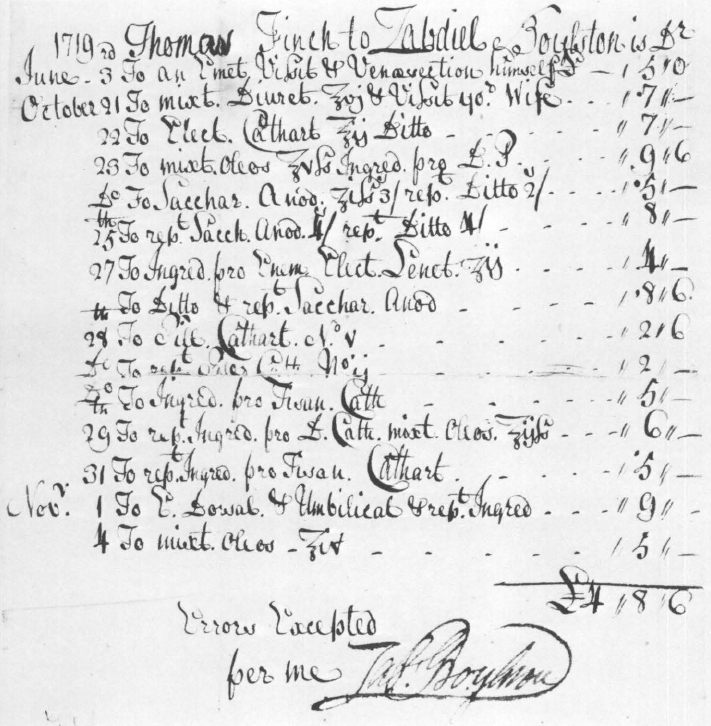
21. Thomas Finch’s account with Dr. Zabdiel Boylston in 1719. The drugs listed can be identified in the Glossary that begins on page 367. Courtesy Boston Medical Library.
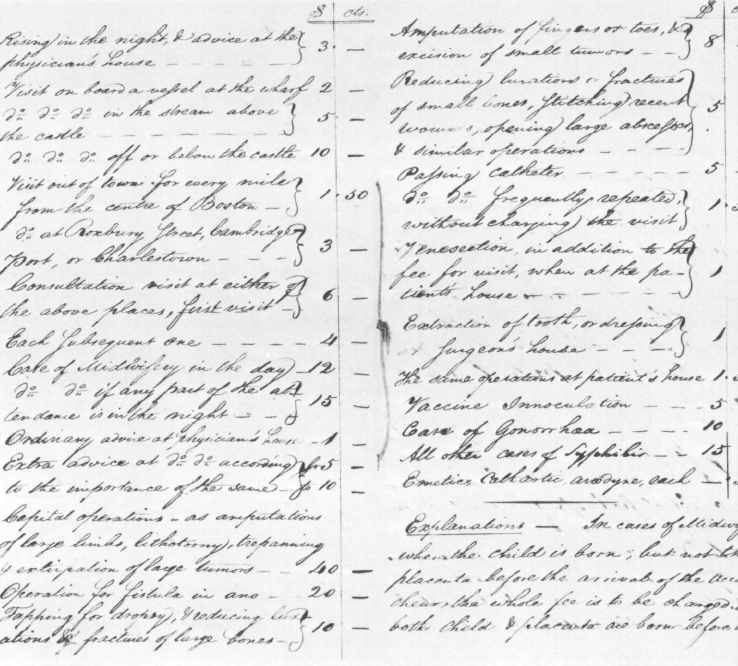
22. Uniform professional medical fees established by the Boston Medical Association, from its manuscript “Rules and Regulations,” February 1806. Courtesy Boston Medical Library.
23. Letter from Dr. Cotton Tufts in Weymouth to his son Cotton, then in school in Concord, describing reactions to the British evacuation from Boston in the past month. Tufts urges his son to acquire professional knowledge “wherever the Means of acquiring it are to be had.” Courtesy Boston Medical Library.
24. Title page of Dr. Benjamin Church’s Boston Massacre commemorative Oration, 1773. Courtesy Boston Medical Library.
25. A Warm Place—Hell, copperplate engraving by Paul Revere, 1768. The poem, by Dr. Benjamin Church, further embellishes Revere’s satirical attack on the seventeen members of the Massachusetts House of Representatives who capitulated to Governor Bernard’s demand that the House rescind its circular letter opposing Parliament’s imposition of taxes on the colonies. The “glorious ninety-two” patriots who defied the governor were, however, in the majority who refused to vote to rescind. Courtesy American Antiquarian Society.
Unless a doctor specified a certain fee in advance, he might have trouble collecting what he thought his services were worth. Before 1770 a jury could lower the fees asked to a “reasonable” level, in the absence of an advance specification. The judges noted that this was a hardship on physicians and that the local practice was contrary to the rules in English cases, two reasons no doubt why the local practice was changed in 1770 to allow physicians to sue for their fees, regardless of any advance stipulation as to the precise amount.10
Naturally, a profession which cannot collect its fees, set its own standards, or escape standards of strict liability for its conduct is not going to flourish. Most professions require the positive support of the government and legal system in terms of approval, exemptions from external regulation, limitations of liability, and implied or express subsidies supporting the operation of the profession. Such legal technicalities and impediments may help to explain why the medical profession in early Boston could not develop sooner than it actually did, but in another sense the technical hindrances were reflections in part of the economic conditions of the colonial period, social practices, cultural attitudes, and political trends as well. Boston, of course, was always a special case, but an exploration of the wider social, economic, cultural, and political context may help to put the plight of the early practitioners in a clearer perspective.
Although our information about the economy and demographic conditions of colonial Boston is by no means complete, it is reasonably safe to say that it was not a healthy place, medically or financially, for a specialized profession to develop and flourish. Some crude approximations of supply and demand tended to minimize the need for sophisticated physicians and the ability of the populace to support anyone solely in the physician’s calling. Boston never exceeded 20,000 people at any time in the colonial period, a limiting factor in how many healers the community could employ or support. One prime ingredient for the encouragement of doctors and proliferation of the medical profession is, of course, a steady supply of sick people who linger long enough to require attention or to hope for a practicable cure. It is clear that Boston was cursed with epidemics of particular virulence and the generally unhealthy conditions of sewage, garbage, rats, and lack of personal hygiene that characterized congested communities in the colonial period. Certainly in that respect there was a need for medical practitioners since there was a steady supply of sick people and, to put it crudely, bumper crops in the epidemic years years after 1720.11 Coincidentally or not, the ministers of the local establishment noted sardonically that illness in the town usually increased after the evangelist George Whitefield’s appearances and revivals before large crowds, which spread disease as well as religious zeal.
Why then did not such miserable conditions provide steady employment for more physicians than actually seems to have been the case? Even without the support of technical knowledge it seems possible that the type of diseases which infested Boston were those that tended to be rather swift in their mortality or recovery and also those which tended to be beyond the specific remedies and state of the art of the profession as it existed. As a result, sick Bostonians might expire very quickly before lengthy treatment was necessary or possible, thus obviating the need for widespread medical assistance. Also, with diseases like smallpox and diphtheria, it appears probable that, once begun, there was not much that could be done beyond normal commonsense precautions, again obviating the need for special professional care. That may explain why some of the physicians sought to promote preventive inoculation rather than rely merely on quarantine after the fact. In addition to those diseases, the accidents that usually accompanied the town’s crafts relating to shipbuilding—broken limbs, amputations, burns—may have been the sort in which commonsense responses of the layman were as adequate as possible under the circumstances without specialized skill. The same may have applied to birth, in which midwives provided all the skill that was possible.12 In short, people in Boston seem to have come into this world and left it without any burning need for regular medical intervention. In between birth and death the usual headaches, stomach disorders, or sprains could be treated with herbal preparations or folk remedies requiring more of the apothecary’s skill than the physician’s or surgeon’s. If people could more or less fend for themselves medically, it would have been difficult for a trained physician to pretend that he could do better or justify any high fee for expert knowledge.
The ability of a population to produce sick people and therefore the need for widespread medical services depend not only upon regular unhealthiness and periodic epidemics. Another way to produce sick people and support doctors is, of course, war. Ghoulish as it may seem, wartime ailments in the form of camp fevers and battlefield injuries have provided a major means by which medical pathology could be studied with a satisfactorily large number of experimental cases and a wide variety of surgical emergencies for the practical training of physicians. Military campaigns, from 1690 to 1715, from 1740 to 1747, and from 1754 to 1760, provided steady work for doctors between periodic epidemics, and it would seem the Revolutionary war gave doctors the impetus to organize, set fees, and gain control over licensing in Massachusetts. But in the earlier eighteenth century, one could argue that wars and military campaigns were not especially helpful to the medical profession, in terms of advancing their knowledge or enhancing their reputation for reliable cures. To be sure, wartime conditions magnified the difficulties of producing relief from camp diseases, but in another sense there were simply not enough wars and military campaigns to provide doctors with a regular practice or opportunities for educational preparation.
Other economic and cultural constraints tended to hinder the entry of talented individuals into the medical profession, as well as the development of organized association among practitioners. The difficulties in gaining enough curable patients, given the health conditions in places like Boston, and in agreeing upon some predictable monetary value for medical services, relate, directly or otherwise, to other general problems of the community. For one thing, until the late colonial period Bostonians generally were too poor to afford regular personal medical attention on a wide scale. A physician therefore might find it difficult to support himself from medical practice alone, if he relied on the usual business of a general practitioner. Second, until the very late colonial period, the local economy was too depressed, limited, and uncertain to produce a comfortable elite class who could act as patrons for physicians or provide a regular system of retainers. Third, while not being total anarchists, Bostonians had a general skepticism of privileged public power in institutionalized form, especially if such institutions cost a lot of the taxpayers’ money. As a result, the voters, who opposed the royal establishment of an executive bureaucracy in government, an established church in religion, and established economic regulation in local or overseas commerce, were far from being enthusiastic about the establishment of medical institutions like hospitals upon which the medical practitioners could organize themselves. Even during the most serious epidemics in Boston, the townspeople allowed temporary public quarantine hospitals only with extreme reluctance, preferring instead the usual (and cheaper) practice of quarantining private homes by use of flags. Even when quarantine hospitals were grudgingly allowed, they were put in the remote corners of west Boston or on islands in the harbor, out of sight and not kept open a moment more than absolutely necessary. The depressed economic conditions in the town for most of the eighteenth century even tended to cut expenses at the almshouse and workhouse to the bare minimum so that they would not become hospitals in the modern or premodern sense of the term.
Thus, the townspeople’s economic values and antagonism to public institutions with privileges militated against any public subsidy of the medical profession in a regular way. And these attitudes were not simply a matter of crude economics and politics. As is most apparent in the long and often violent opposition to smallpox inoculation, there were cultural and intellectual biases against the arts of healing as a legitimate calling in the community. If, as seems to be the case, popular religious feeling tended to equate disease with divine providence and divine judgment, then the physicians who dared to tamper with God’s plan skated close to the edge of heresy and blasphemy. Even for those enlightened souls who did not believe the religious explanation of disease, individuals like Benjamin Franklin and William Douglass gave the impression that innovations in medical cures or preventive medicine violated the laws of enlightened reason, calculated self-interest, and the other theories of natural law in the eighteenth century. Bostonians did not often go to the extremes of attempting to assassinate Cotton Mather for advocating inoculation, but their religious fatalism or skeptical rationalism combined with other attitudes about political economy to make medical practice and medical experimentation appear to be abnormal deviants from accepted cultural and intellectual standards in the social community.13
In a related way other cultural and intellectual trends served to reinforce popular skepticism of medical specialization and professionalization. For religious purposes, local authorities were expected to encourage literacy through schooling, one of the few public institutions permitted to exist at public expense aside from regular churches. Bostonians seemed rather avid readers, enough to subsidize several newspapers and booksellers, more so than in other communities of comparable size at the time. As a result, rudimentary medical information and medical literature were accessible to the lay public and not just affordable or comprehensible by a specialized elite of physicians, with specialized jargon and arcane monopolies of expertise.
All of these economic, political, social, and intellectual factors may help to explain why individual physicians and the medical profession in general faced almost insuperable obstacles in a colonial community like Boston. This is not to say, however, that doctors were negligible or nonexistent in the town. Other papers in this volume trace the particular contributions of individual physicians and the minute seeds of later professional organization. What strikes the nonmedical historian about Boston’s physicians is the familiar fact that they fit in very well with the patterns of occupation, specialization, and professionalization experienced by other skilled craftsmen and practitioners in the community. We know in general how important colonists in New England revered the complex attributes of the work ethic and the idea of calling. In one sense such notions militated against most specialized professions (except, of course, the clergy) since the practitioners of medical or legal arts and crafts had the burden of proving to the community that they were legitimate, productive callings beneficial to the public. Lawyers especially had difficulties convincing anyone that their talents deserved public approval or high fees. For the reasons given above, physicians too had a hard time proving their worth either in terms of the intrinsic legitimacy of their calling or in terms of practical improvements and accomplishments.14 As long as high mortality and other socioeconomic conditions gave people the commonsense notion that people would die no matter what medical service was at hand, the doctors had little means to argue that having physicians and medical help was better than not having them, or that it might be cheaper in the long run to support medical improvements, experimental though they might be, rather than do without them in a short-run reliance upon divine providence.
One intriguing result of these difficulties was the familiar fact that doctoring tended to be a part-time sideline of educated or skilled people in other, more socially acceptable, callings, like ministers who took some notice of the physical as well as the spiritual welfare of their flocks. What is even more striking to me is the number of political leaders who were also full-time or part-time physicians. Before 1740 Thomas Oakes, William Clark, Oliver Noyes, and Elisha Cooke Senior and Junior, politicians who helped to create the Boston Caucus as the country’s first urban political machine, were known as physicians as well as landlords and merchants. In the period after 1740 William Douglass, Joseph Warren, Thomas Young, and Benjamin Church were physicians with wide political influence. In a sense, physician-politicians more consistently provided the leadership of popular politics than did lawyers, teachers, merchants, or other skilled craftsmen. As physicians in part, these political leaders were highly visible in the town and earned a reputation for sensitivity to issues affecting public welfare. It is hard to think of similar physicians who played comparable roles for the royal establishment. Political action was perhaps one way in which individual physicians could counteract the monopoly of professional influence exerted by the town’s organized clergymen, and it helped to hasten the erosion of clerical power in the late colonial period when lawyers, merchants, teachers, and physicians joined together to promote popular causes as well as their own legitimacy as accepted equals of the clergy.15 Consequently, given all the impediments to the advancement of professional healing as an accepted calling in its own right, and the part-time nature of medical practice, the political, nonmedical alliances of the town’s physicians helped to contribute not only to challenges against the royal establishment during the Revolution, but, at the same time, to their own development as an organized professional specialized institution. In the postwar period, without many of the previous impediments to corporate organization, the physicians, like other special-interest groups, were able to incorporate themselves, set fees, establish standards, control licensing, limit their legal liability, and, in short, to lay the foundations for modern businesslike development.