WILLIAM C. WIGGLESWORTH
WILLIAM C. WIGGLESWORTH 
Surgery in Massachusetts, 1620–1800*
IN 1962 I was asked, as Medical Examiner, to identify some bones found by boys playing in a gravel pit in Ipswich, where I live and practice surgery. Carbon-dated at the Peabody Museum in Cambridge, the bones proved to be at least 300 years old, relics of an Indian burial ground. They included vertebral bodies of all sizes, numerous mandibles and carpals—and a well-healed fractured femur that led me to believe that the Indians knew how to set fractures.
My office in Ipswich is near Giles Firmin Park. Twenty years ago it was a beautiful open space in which Saltonstall Brook was shaded by willows. Now Town Meeting has turned it into a well-worn playground; the willows are gone, and the brook has been reduced to a pipe. Ipswich voters seemed not to know much about Giles Firmin except that he was a physician;1 they referred to him familiarly as “Giles.”
These two unrelated incidents, and my own curiosity, led me into historical research. It has been the search of an amateur, not a trained historian. It has been fascinating, and often rewarding, to have found what I have in libraries and early records. It has been equally frustrating to encounter gaps in our knowledge of American medicine and surgery in the distant past. For example, references to “John Aniball, a good dresser of wounds,” and to Dr. Philami Daws, who “ministered well to fleshy ills,” do not include the surgical methods that prompted those accolades.2 Records of the early colonial period contain few, if any, precise descriptions of contemporary surgical procedures and techniques, but certain patterns of professional practice do emerge from even the fragmentary sources available.
When Deacon (although he was called “Doctor”) Samuel Fuller3 and three barber-surgeons arrived on the Mayflower in 1620—Fuller to establish a busy practice from Salem to Plymouth, and the three barber-surgeons to return to England a year later4—they brought with them the medical theories and traditions of Europe. However, they soon learned techniques practiced by local Indians, such as isolating their wounded and splinting fractures with wood or with wet pieces of leather that shrank when dry to form a splint.5
In England at that time Galen’s concept of disease still dictated most medical treatment.6 He had postulated not that disease was specific, as we believe today, but that it represented disturbances among the four humors (blood, phlegm, black bile, and yellow bile). Therefore, appropriate cures would result when the balances were restored, for example, by bleeding, purging, or sweating. Bloodletting would not fall into discredit until the nineteenth century.7
Galen had advocated cleaning clots and foreign material from wounds before suturing them as long ago as the second century. He felt that suppuration, or “laudable pus”, favored effective healing. Throughout the Middle Ages a few surgeons, like Theodoric, at Bologna, noted that “such a practice [the promotion of suppuration] is indeed to hinder Nature, to prolong the disease and prevent the conglutination and consolidation of the wound.” But such lessons were forgotten, if they had ever been learned, among colonial physicians, who were relieved when their patients’ wounds produced optimum amounts of pus.8
Only slowly did newer, non-Galenic concepts cross to the New World. By the time Samuel Fuller arrived in Plymouth, Paracelsus (1493–1541), for example, had argued that disease should be treated with purified chemicals, such as laudanum, mercury, arsenic, and lead. Ambroise Pare (1517–1590) had newly introduced the technique of covering wounds with bland mixtures, rather than the traditional boiling oils.9
The three barber-surgeons who accompanied Dr. Fuller reflected the relatively low status of some early surgeons, regarded as adjuncts to the physician. Their practice was limited to treating the outside of the body; they were prohibited from invading it. Public respect for their profession was slight until a much publicized operation cured Louis XIV of his fistula in ano in 1686.10
In early colonial times the word “physician” did not imply the precise definition we accept today. Some practitioners were educated, some not. Some were ministers. Only a few had earned M.D. degrees at European medical schools.11 Steeped in the Puritan ethic, and in an absolute belief in the supernatural and a fierce and unforgiving God, the minister-doctor combination is exemplified by Cotton Mather, who portrayed the two professions in “an angelic conjunction.”12
Another example from an even earlier time is Giles Firmin, whose park is now deteriorating. Born in England in 1615, he arrived in Massachusetts in 1630, where he practiced medicine as well as surgery and dentistry. Interested in anatomy and physiology, he trained many successful apprentices, including Dr. Thomas Barry who, in turn, taught Dr. Edward Augustus Holyoke (1728–1829), the first president of the Massachusetts Medical Society. Two centuries later, Oliver Wendell Holmes would use Firmin as a model of good clinical judgment.13
Firmin’s insistence on the necessity of accurate anatomic knowledge led him, in 1647, to argue that the General Court should pass a resolution providing that “such as studies of physick or chirugery may have liberty to reade anatomy, and to anatomize once in foure years some malefactor in case there be such, as the Courte shall afford of.” Nevertheless, not until 1834 would the General Court legalize dissections of unclaimed bodies, at the urging of the Massachusetts Medical Society.14
Firmin often extracted teeth, but his attempts at making dentures were not always successful. For example, a farmer for whom he had made a wooden denture was unable to pay cash, so they settled on a new hay rake for the doctor. However, as the summer wore on it became obvious that the teeth of the rake were made of green wood. As they dried, so the story goes, they fell out, like those Firmin had made for his patient’s mouth.15
Firmin finally gave up. He and Mrs. Firmin decided that he could not make a living here, so they returned to England in 1647, after the doctor had presented his arguments for legalizing anatomic studies. On his return to England, he gave up medicine but continued his ministry. Later, expelled from his church for unknown reasons, he returned to medicine, surgery, and dentistry until his death in 1697.16
Surgery was sometimes practiced by ferrymen, farmers, shipmasters, lawyers, tailors, tavern keepers, and cordwainers, among others, as the need arose. Because patients’ needs for operations were infrequent, surgery was not a full-time job, and cohesive professional focus and growth were slow. Although most practitioners depended on both Galen and luck, a few tried to reason from cause to effect. The thinking of some early doctors provides delightful reading. For instance, Cotton Mather reported that “Abigail Eliot lost part of her brain in an accident. Those which remained thereafter swelled with tides. Yet with insertion of a silver plate in her head, she lived happily ever after.” Sarah Wilkinson “died of dropsy and was found to have lived for years with almost no internal organs whatsoever.”17
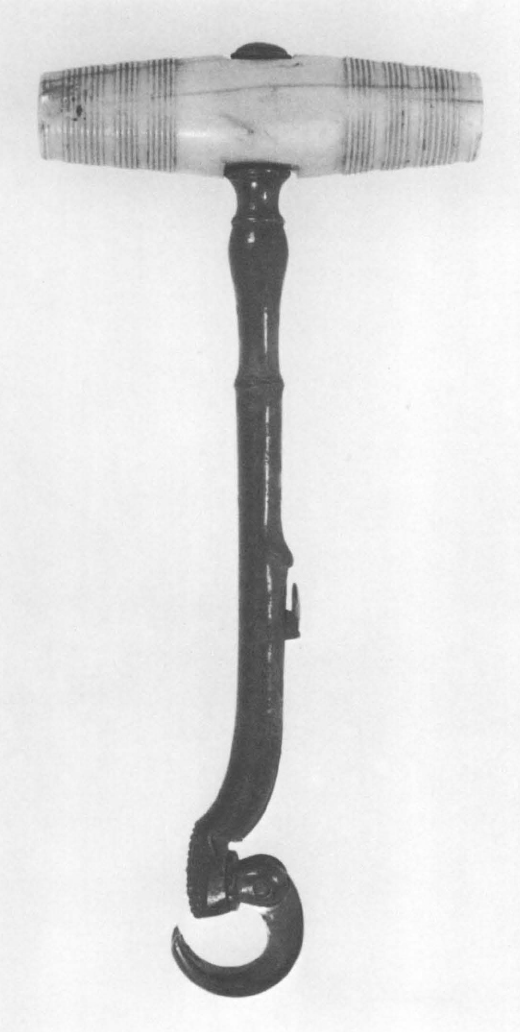
44. Tooth extractor (also called a turnkey or pelican), eighteenth century. The tool’s claw was engaged with the patient’s tooth in such a way that it could be removed by twisting the tooth in its socket to free it from the ligaments suspending it there. Photograph by David Gunner. Courtesy Boston Medical Library.
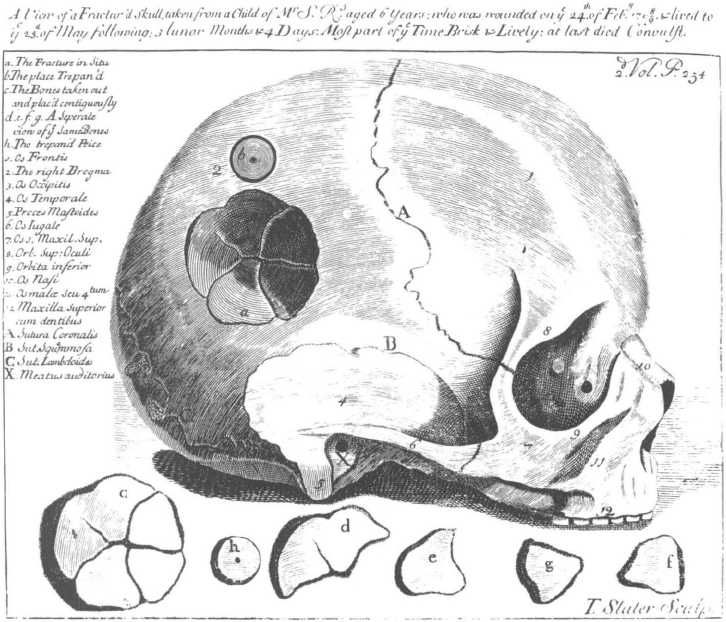
45. “A View of a Fractur’d Skull” from Daniel Turner, The Art of Surgery, 2nd edition (London, 1741). Courtesy Boston Medical Library.
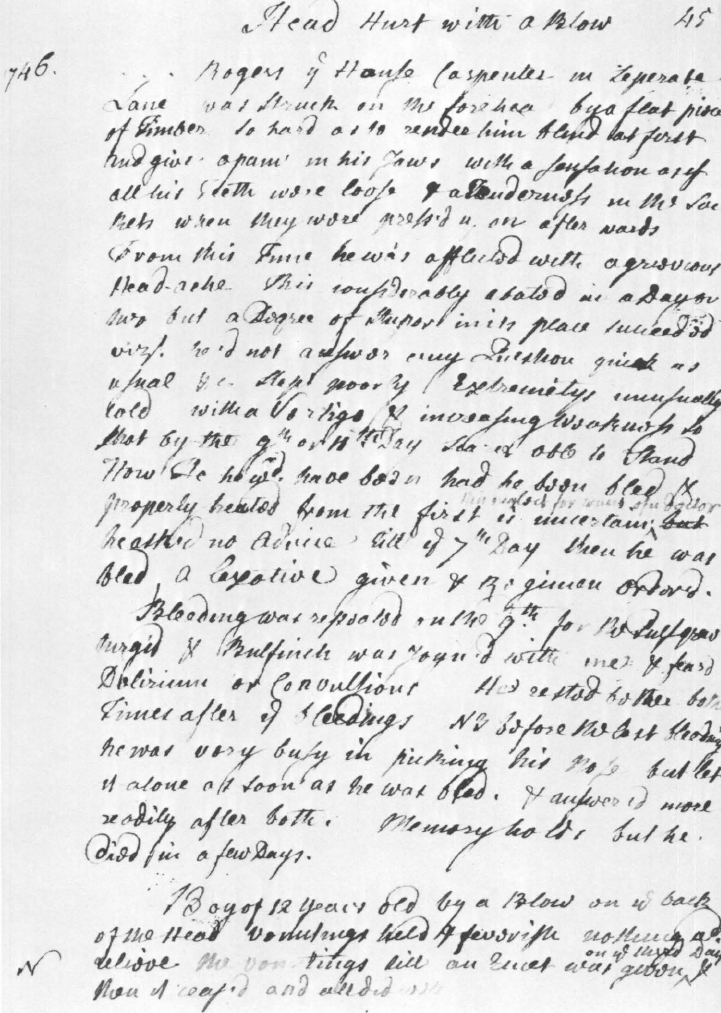
46. Surgical notes of Dr. John Perkins (1696–1781). This 1746 note, concerning the unsuccessful treatment, by bleeding him, of a man struck on the head by a large hewn timber, is in Perkins’s unpublished ms “Observations Medical & Chirurgical.” Courtesy Boston Medical Library.
There was little opportunity for professional communication among the earliest colonial practitioners. News of their successes and failures spread by word of mouth, and there was little chance for individual professional growth except by trial and error.18 Many books brought from Europe were in Latin. And until 1674 Charles II allowed only one printing press in Massachusetts, which had been set up in Cambridge in 1639. Not until 1704, when the Boston News-Letter began weekly publication, did the distribution of medical and surgical information even begin to increase. For example, a News-Letter of 1710 reports the successful removal of a bladder stone “of considerable bigness” from a child; Dr. Zabdiel Boylston “with the blessing of God and in less than a month’s time has perfectly cured him and [he] holds his Water: This is the third Operation performed in the Stone on Males and Females.”19 Many other periodicals, almanacs, and books began to appear later, along with increasingly clear descriptions of actual techniques and surgical procedures. For instance, several detailed accounts of operations performed by Dr. Hall Jackson of Portsmouth were reported in the New Hampshire Gazette, including excellent descriptions of cataract surgery and amputations.20
The effort for formal organization and exchange of ideas began to take positive form in 1735 when Dr. William Douglass (1691–1752) wrote to Dr. Cadwalader Colden (1688–1776) of New York,“... we have lately in Boston formed a medical society.” Douglass went on to describe a projected first volume of Medical Memoirs, for which five papers were planned, but it was never published.21
At the outbreak of the Revolution several very practical books on operative surgery were published to assist army surgeons in the field. An Austrian volume on The Diseases Incident to Armies with the Method of Cure, by Baron Gerhard van Swieten (1700–1772), was republished in Philadelphia in 1776. He said that hemorrhage from the nose need not be treated until “the pulse begins to undulate, and the face and lips grow pale.... The means of stopping it are, applying bandages to the arms and thighs of the patient, because the veins being thereby compressed, the reflux of the blood to the heart is in less quantity. The Haemorrhage stopped, the bandages are not to be loosened all at once, but successively one after another, in such a manner as to leave the space of a quarter of an hour between the loosening of each bandage.”22 This seems to be one of the earliest suggestions that tourniquets can reduce the work of the heart. The technique of rotating tourniquets is still used occasionally for treating congestive heart failure, but not, as far as I know, for nose bleeds!
However, should this technique fail, “Let a tent of lint imbibed in the styptic No. 56 be put up that nostril from which the blood came. If some lint dipped in the stiptic be wrapped round a quill, it will be easily introduced up the nose... where it is to remain for a day or two, till it falls out of itself.”23
Extracts from British army medical manuals were printed along with van Swieten’s text for the benefit of Continental Army surgeons. One of these was William Northcote’s discussion of wounds of veins, arteries, nerves, and tendons. He had pointed out that “In wounds of the Veins, the blood flows with a smooth even stream, of a gross consistence and dark color; and is ordinarily restrained by the common methods, such as dry lint, styptics, &c.”24
However, “If an Artery is wounded, the blood flows impetuously and ... is of a florid color; to suppress which, if the orifice be accessible, make a ligature on the Artery.... [However,] if it be not accessible, and the Artery runs along the side of a bone, apply a suitable bandage, compress, or bolsters,” but not so tightly as to occlude blood flow completely, so that a clot will be able to form. Only if the artery lies within a bone where it cannot be compressed should dry lint be applied to staunch its flow forcibly. Styptics and cauteries were never appropriate when ligatures or compression were feasible.25
If tendons were wounded, they were to be splinted, but not sutured, to avoid suppuration, which would tend to shorten them. If major nerves were completely severed, the limb would have to be amputated, because the arteries below the cut would not be able to function without their nerve supplies. However, nerves that were only partially severed could be expected to heal after Peruvian Balsam had been poured into the wound.26
The first native American textbook of surgery was John Jones’s Plain Concise Practical Remarks on the Treatment of Wounds and Fractures, republished in 1776 along with van Swieten’s. Referring back to Hippocrates’s opinion that surgeons and physicians were professional equals, Jones (1729–1791) saw no reason why a surgeon should be a technician overseen by a physician, much less why this tradition should continue in America. Rather, a surgeon should know about all illnesses, but have mastered the operating techniques needed to relieve disease.27
Jones provides many detailed instructions for treating different kinds of wounds; incised, punctured, lacerated, and contused. Techniques like his are used today, including debridement, excision of jagged wounds to convert them into incised wounds, and dilating puncture wounds, rather than closing them. Other wounds should be closed with “sticking plaster” and sutures if necessary, after drawing the lips of the wound together without puckering or wrinkling them. Sutures should be kept to a minimum, and, after two or three days, followed by adhesive plasters. Contused wounds were different; because the blood vessels had been destroyed, suppuration would follow, so Jones advocated dependent drainage for their treatment. Unfortunately, he concluded that “I scarcely need observe, that moderate evacuation, by bleeding, and gentle purging, together with a low diet, are, in these cases absolutely necessary.”28
He considered all thoracic and abdominal wounds as essentially mortal. However, some would survive according to the severity of the wound, provided that the patient or his physician committed no errors which would increase the degree of fever or inflammation. Jones recommended that if gangrenous abdominal fat protrudes it should be excised and the wound closed.29
He treated simple fractures by reducing them and placing the limb in a splint so that the stresses on opposing muscles could be equalized. He admonished against treatments which would cause the severed bones to “rise.” If that should happen, the position of the splints should be changed, to minimize the forces pulling the bone out of line.30
The treatment of compound fractures was more controversial. Although some surgeons of Jones’s time advocated amputation, others felt it was not necessary. They recommended removing foreign material from the wound, and applying soft dry lint to permit free drainage and promote a speedy suppuration. Cautious bleeding, to draw off inflammation, was also recommended. If drainage were excessive, amputation should then be considered.31
Amputations had been done for many years. An earlier French method was crude by any standard. The limb to be amputated was placed across two vertical boards. The surgeon fractured the bone with one blow of a narrow sledge. Dropping the sledge he then reached for his knife and cut the soft tissue, applied a cautery to the stump, bandaged it, and sent the patient home.32
Jones introduced his description of the progress made since that method had been used with the following admonition: “As every operation is necessarily attended with a certain degree of bodily pain ... a good surgeon should be in the first place well assured of the necessity of an operation, before he proceeds to perform it, and secondly he ought to consider, whether the patient will in all probability be better for it, or whether he may not be the worse.” By this time amputations had become more sophisticated. Skin and muscle flaps were made, and the bone was cut with a saw. Planning for suitable and comfortable prostheses was becoming more routine.33
The earliest Massachusetts Medical Society records contain many interesting accounts of specific operations and how they were performed in the last two decades of the eighteenth century. Seth Field of Hardwick reported an operation he performed on a baby with an imperforate anus. He incised the perineum, and, with blunt finger dissection, went as far as he dared without entering the peritoneum, but no excrement appeared. Following the operation the baby was given a laxative, whereupon fecal matter soon came from the penis. At autopsy three days later, the colon was found to enter the bladder in coffee-spout fashion. Jean Feron, “first Chirurgion & Physician of the French Fleet in North America,” submitted three very vivid reports of attempts to treat skull fractures. Although the patients responded well at first to irrigation of the spaces below their wounds, fever and pus finally appeared, and all three men died. Nevertheless, the paper was read at a society meeting in 1788. Thomas Babbitt, in Sturbridge, reported that he had reduced an abdominal fat pad (omentum) that had been incarcerated for thirteen days by removing the gangrenous layer of fat through a daring abdominal incision. The patient was able to resume his usual activities within seven weeks. And William Lyman of York, in the District of Maine, treated a woman with an incarcerated umbilical hernia that had caused intestinal obstruction with calomel, castor oil, narcotics, and tobacco enemas. After fourteen days of these medicines, the hernia had softened, the patient had stopped vomiting feces, and she had a normal bowel movement.34
These manuscripts fascinate us today as much as they must have the Massachusetts Medical Society audience for whom they were intended; they are much more frightening to us, but for a different reason. That is, we can only look back with horror on the colonial surgeon’s inability to prevent pain effectively. The only pain-killers available to him were opium (often administered as laudanum, an alcoholic extract of opium), Indian hemp, alcohol, water hemlock in small doses, bilateral carotid pressure, and tourniquets applied so tightly as to numb the nerves. In addition, the patient could also usually manage to faint as he was being cut.
Surgery in the days before general anesthesia was introduced in 1846 was described, by one of its eminent eighteenth-century practitioners, as “long and murderous... when the surgeon labors for an hour in extracting the stone, to the inevitable destruction of the patient.” A later observer probably did not overdramatize when he wrote that “Every now and then there was a cry of ‘Hush!’ which was succeeded by the stillness of death, broken only by the horrible squash, squash, of the forceps in the perineum. ‘Oh! let it go—pray let it keep in!’ was the constant cry of the poor man.” Stone operations, or lithotomies, often could be completed in only a minute or two, but they were always painful to some degree.35
Or consider the physician who himself had to undergo an amputation. The physician-patient agreed to the operation if he could have time to prepare for the death that he thought was inevitable. When the time came, the operation took longer than he had anticipated, or at least it seemed to take longer. “It necessitated cruel cutting through inflamed and morbidly sensitive parts, and could not be despatched by a few strokes of the knife.... Suffering so great as I underwent cannot be expressed in words.... But the blank whirlwind of emotion, the horror of great darkness, and the sense of desertion by God and man ... I can never forget, however gladly I would do so.”36
Even the patient who was himself a doctor was nonetheless horrified at what he saw his own surgeon do: “During the operation, in spite of the pain it occasioned, my senses were preternaturally acute, as I have been told they generally are in patients under such circumstances. . . . I still recall with unwelcome vividness the spreading out of the instruments, the twisting of the tourniquet, the first incision, the fingering of the sawed bone, the sponge pressed on the flap, the tying of the blood-vessels, the stitching of the skin, and the bloody dismembered limb lying on the floor.”37 His experience points up the other great benefit conferred by anesthesia, in addition to the relief of the patient’s pain: it permitted the surgeon to approach his patient’s particular problem more slowly, carefully, and methodically than ever before possible. Before 1846, many operators, as well as their patients, must have wished they had never thought of surgery.
I have quoted from these pages at length to illustrate some graphic, but reasoned and educated, views of the horrors and pain to which colonial surgical patients were subjected. Under such appalling conditions, it is understandable that, in the first century, Celsus had stressed that it was essential for an operative surgeon to be without pity. I feel that most of these trained and untrained surgical practitioners knew what had to be done, that they sympathized with their patients’ suffering, and that they did their best to operate quickly, to heal surgical wounds, and to rehabilitate their patients.
During the Revolutionary war, as in all wars, great strides were made in techniques for treating wounds of the abdomen and chest, but subsequent infection precluded any real improvements in postoperative mortality and morbidity. Surgeons had gone about as far as they could go without understanding the nature of infection and without anesthesia.
During the colonial period, then, men with very little formal training in surgery, and with no systematic means of professional communication, were doing surgical procedures—some that were centuries old, some that were indigenous to the Indians, and some that were designed on the spot to meet immediate specific needs. As Galen’s theories gradually disappeared, bleeding finally could begin to follow suit. These early surgeons depended on speed, brute strength, and optimism. Yet behind their sometimes barbaric and ruthless efforts one feels that they were dedicated, God-fearing men. As John Jones wrote in the dedication of his book on wounds to Dr. Thomas Cadwalader, his and their lives “were ones of continued scenes of benevolence, and humanity, the most feeble efforts to soften human misery and [to] smooth the bed of death.”38
Some Eighteenth-Century Surgical Tools and Techniques
The following plates and text, except where specified otherwise, are taken from [Henri François] LeDran, The Operations in Surgery, trans. by [Thomas] Gataker, and with plates by [Dr. William] Cheselden, 3rd ed. (London, 1757). (Courtesy of Boston Medical Library.) This book was owned, and presumably consulted, by at least several late eighteenth-century New England surgeons.
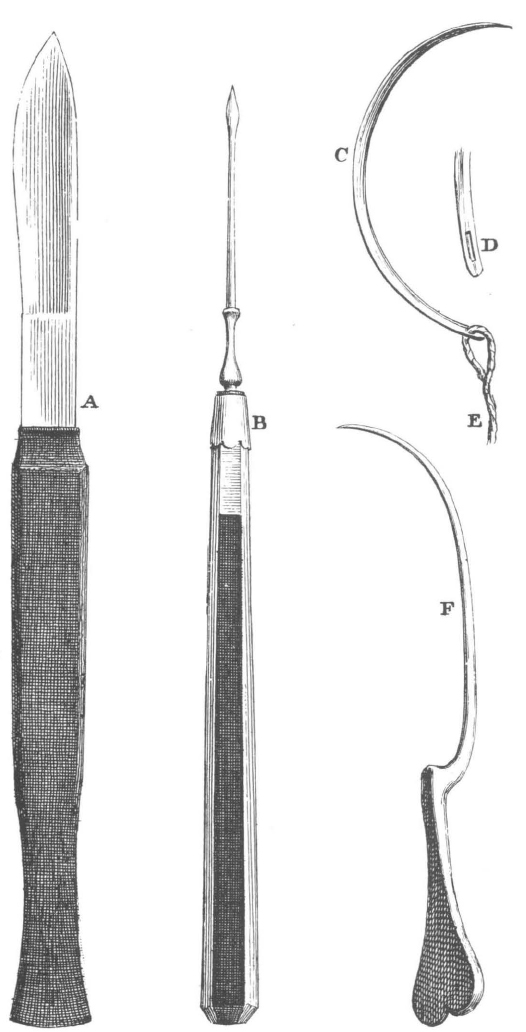
47. Surgical instruments, plate xiii in LeDran’s Operations in Surgery. See facing page for his description. Courtesy Boston Medical Library.

48. Surgeon’s kit, eighteenth century. See text on facing page for description and for LeDran’s recommendations. Photograph by David Gunner. Courtesy Boston Medical Library.
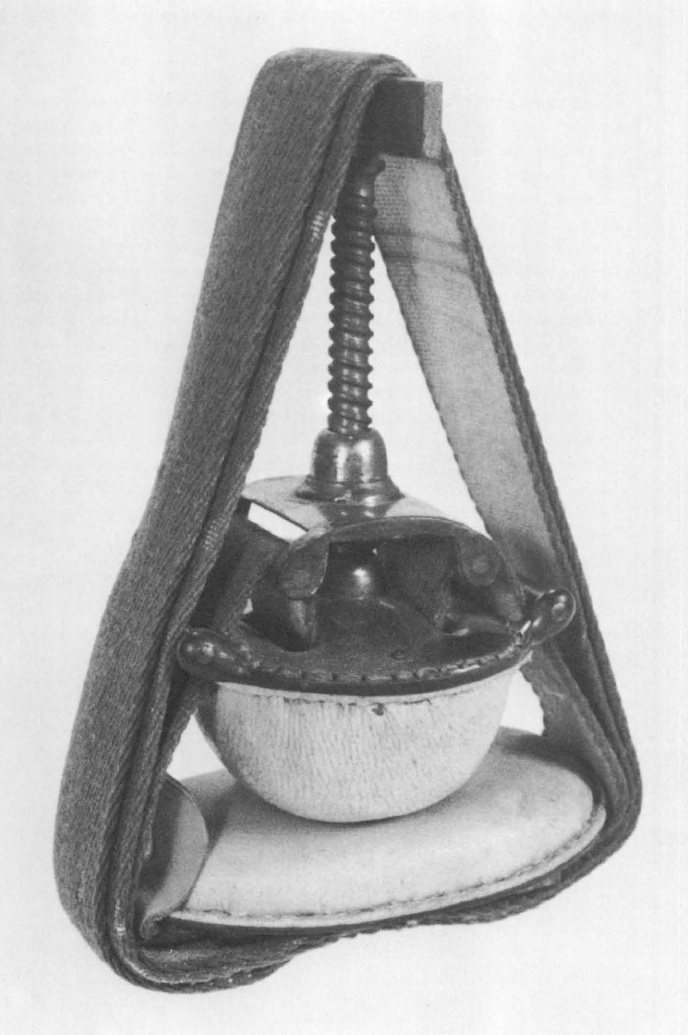
49. Tourniquet, eighteenth century, from kit in preceding illustration. See text on facing page for description and for LeDran’s recommendations. Photograph by David Gunner. Courtesy Boston Medical Library.
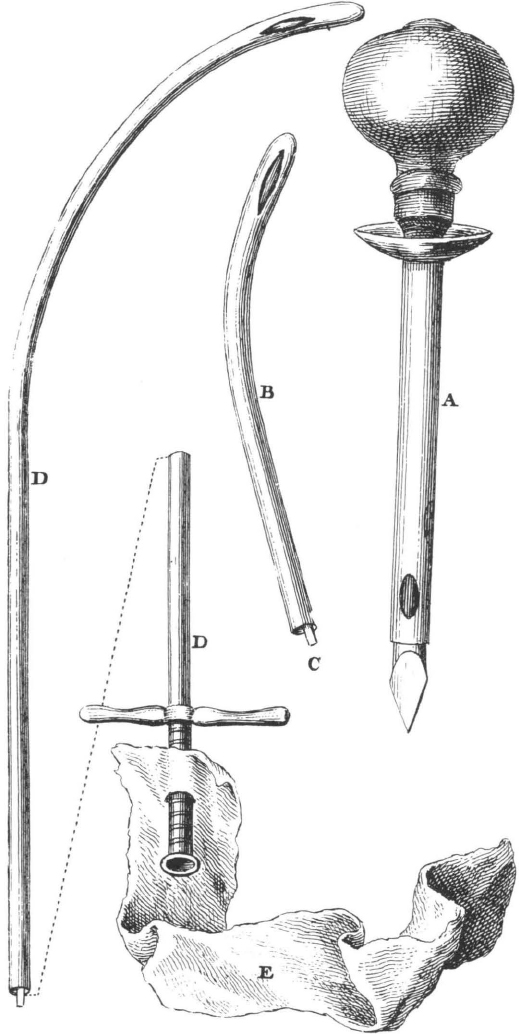
50. Catheters, plate xiv in LeDran’s Operations in Surgery. See facing page for his description. Courtesy Boston Medical Library.
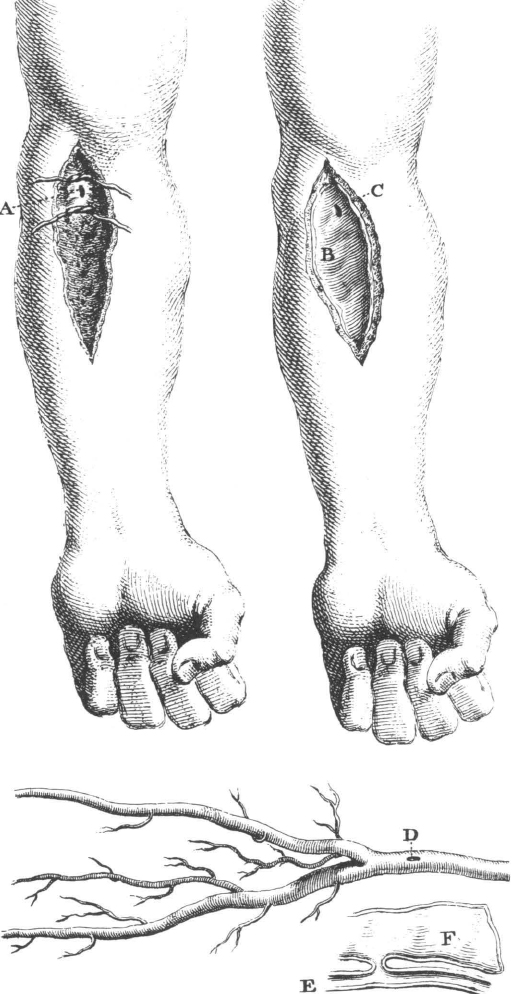
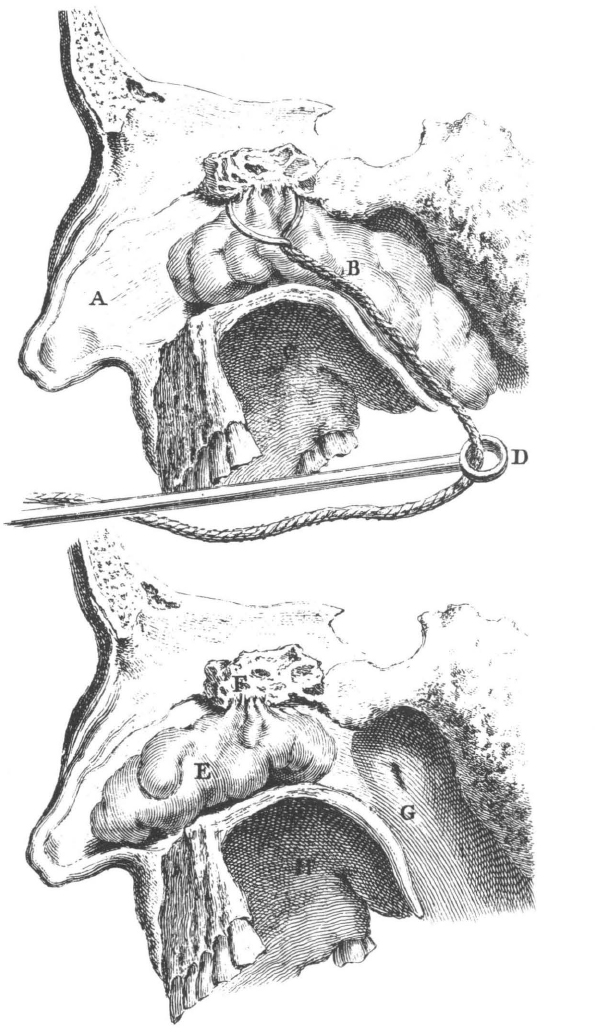
51. Treatment of aneurysm of humeral artery, plate xii in LeDran’s Operations in Surgery. See text on facing page for his description. Courtesy Boston Medical Library.
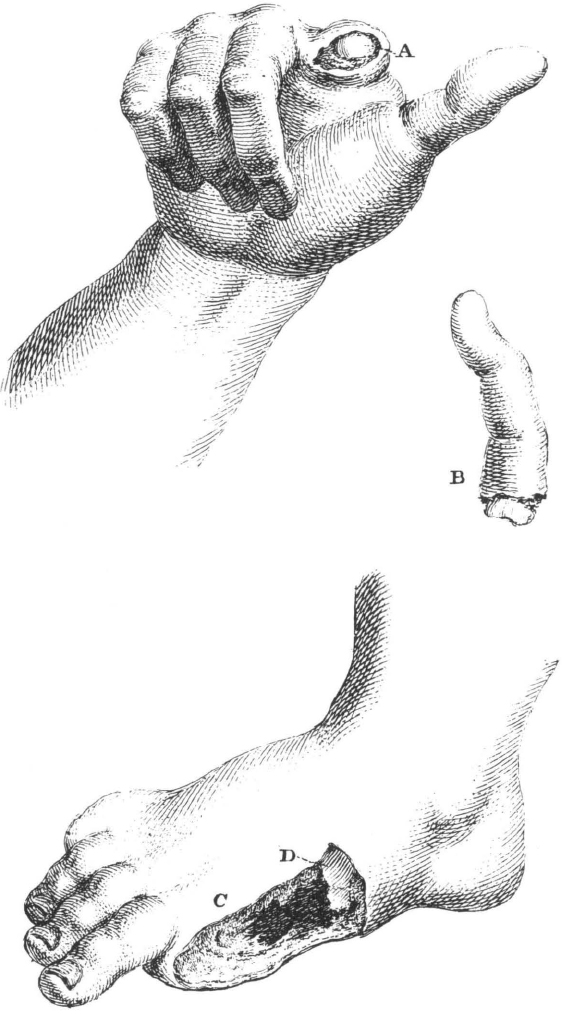
52. Finger and toe amputations, plate xvii in LeDran’s Operations in Surgery. See text on facing page for his description. Courtesy Boston Medical Library.
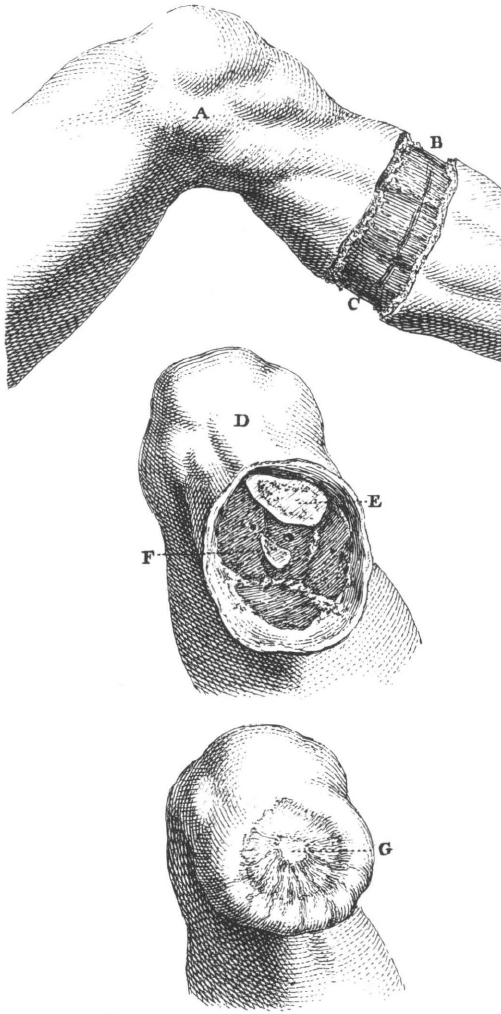
53. Mid-calf leg amputation, plate xix in LeDran’s Operations in Surgery. See text on facing page for his description. Courtesy Boston Medical Library.
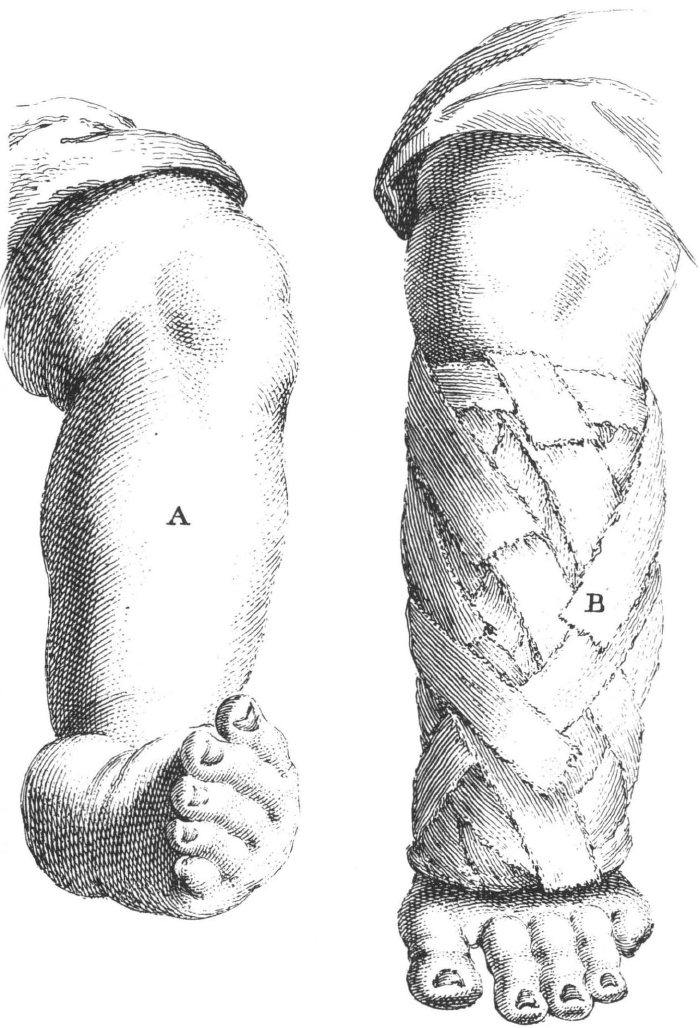
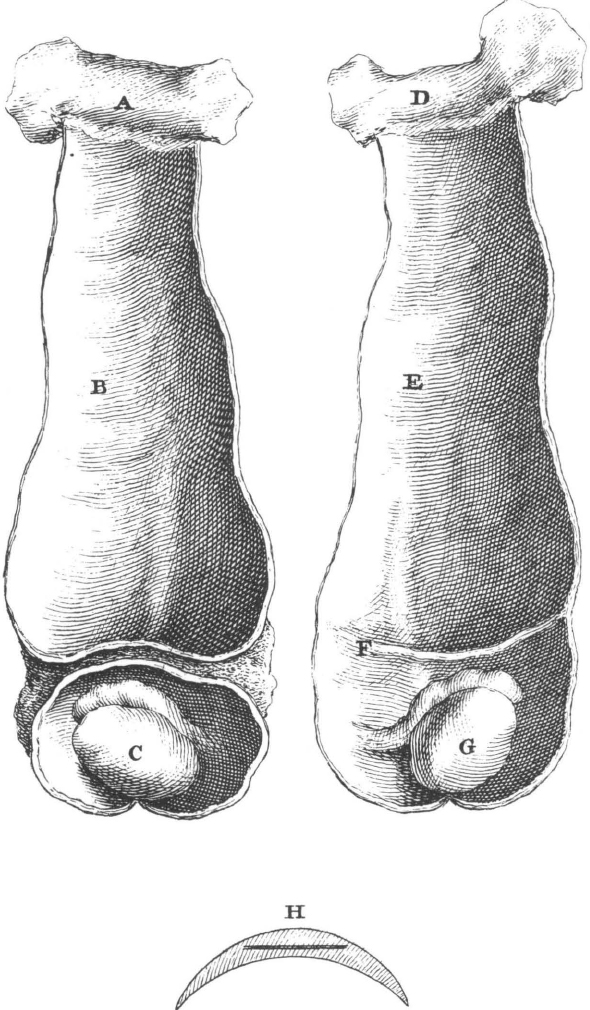
54. Treatment of clubbed foot, plate vii in LeDran’s Operations in Surgery. See text on facing page for his description. Courtesy Boston Medical Library.